Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
surgery
If there is continuing and significant ocular irritation despite optimal medical therapy, then surgical intervention is indicated. Typically such procedures are performed under local anesthesia.
Simple excision is the most straightforward technique, but recurrence rates >33% have been reported.[19]
Conjunctival autografting and flaps is the most commonly used surgical technique and involves covering the bare scleral area created following pterygium excision with either rotational conjunctival flaps above and/or below or with a free conjunctival graft taken from the superior bulbar conjunctiva. [Figure caption and citation for the preceding image starts]: Eye following pterygium excision and conjunctival autografting 1 day after surgeryFrom personal collection of David O'Brart; used with permission [Citation ends].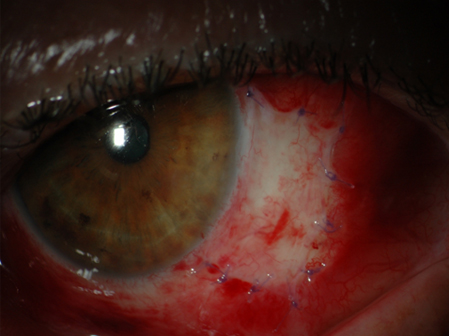 Recurrence rates after conjunctival autografting techniques are encouraging.[20][21][51]
[
Recurrence rates after conjunctival autografting techniques are encouraging.[20][21][51]
[ ![]() ]
]
With an extensive pterygium or in glaucoma patients, amniotic membrane transplantation may be used to cover the bare scleral area.[27][30]
Lamellar keratoplasty (partial thickness corneal transplantation) may be required if corneal thinning is significant, or with very aggressive or recurrent cases.
Excimer laser phototherapeutic keratectomy (PTK) may be a useful adjunctive treatment in aggressive cases involving the visual axis.
Redirection of the head of the pterygium has been abandoned due to high recurrence rates.
surgery
There are several surgical techniques, depending on the characteristics of the pterygium. Typically such procedures are performed under local anesthesia.
Simple excision is the most straightforward technique, but recurrence rates >33% have been reported.[19][51]
Conjunctival autografting and flaps is the most commonly used surgical technique and involves covering the bare scleral area created following pterygium excision with either rotational conjunctival flaps above and/or below or with a free conjunctival graft taken from the superior bulbar conjunctiva. [Figure caption and citation for the preceding image starts]: Eye following pterygium excision and conjunctival autografting 1 day after surgeryFrom personal collection of David O'Brart; used with permission [Citation ends]. Recurrence rates after conjunctival autografting techniques are encouraging.[20][21]
[ ![]() ]
]
With an extensive pterygium or in glaucoma patients, amniotic membrane transplantation may be used to cover the bare scleral area.[27][30]
Lamellar keratoplasty (partial thickness corneal transplantation) may be required if corneal thinning is significant, or with very aggressive or recurrent cases.
Excimer laser phototherapeutic keratectomy (PTK) may be a useful adjunctive treatment in aggressive cases involving the visual axis.
Redirection of the head of the pterygium has been abandoned due to high recurrence rates.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer