Tests
1st tests to order
CBC and differential
Test
Leukocytosis and thrombocytopenia in the absence of disseminated intravascular coagulation in the acute/initial phase. May show anemia secondary to hemorrhage in the immune phase.
Result
high WBC count; low platelet count; anemia
urinalysis
Test
Should be ordered in all patients in the acute/initial phase.
Result
mild proteinuria; pyuria; hematuria; hyaline or granular casts
microscopic agglutination test (MAT)
Test
MAT paired acute and convalescent sera taken 2 weeks apart.
Result
fourfold increase between acute and convalescent sera is diagnostic
enzyme-linked immunosorbent assay (ELISA)
polymerase chain reaction (PCR)
Test
Can provide a more timely diagnosis during the acute phase, if available. Can be amplified from serum, urine, aqueous humor, and other tissues; however, the best specimen is serum. The transience of leptospires in body fluids means that a negative PCR test does not exclude leptospirosis.[56]
There is substantial variability between studies assessing the accuracy of PCR and real-time PCR, and it is uncertain whether PCR or real-time PCR is better in detecting leptospirosis. There is preliminary evidence that PCR is more sensitive on blood samples collected early in the disease course.[57]
[ ![]() ]
]
Result
positive for Leptospira DNA
darkfield examination
Test
Direct visualization of spirochete in blood or urine specimens. Likely to be positive during acute/initial phase. Darkfield examination has poor sensitivity and specificity.[Figure caption and citation for the preceding image starts]: Microscopic agglutination test with live antigen using darkfield microscopy techniqueImage provided by the CDC and the Public Health Image Library [Citation ends].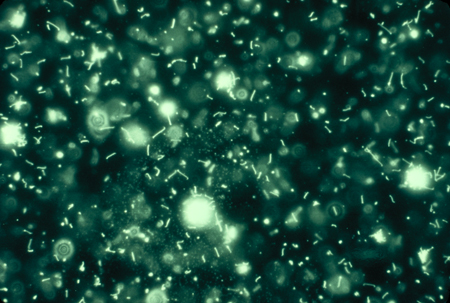
Result
presence of spirochetes
blood culture
Test
Leptospires can be isolated from blood during the first week to 10 days (acute/initial phase). Culture is insensitive and slow and is therefore not recommended as the sole diagnostic method.[50]
Result
positive after 1 week to 4 months
cerebrospinal fluid (CSF) culture
Test
Leptospires can be isolated from CSF during the first week to 10 days (acute/initial phase). Culture is insensitive and slow and is therefore not recommended as the sole diagnostic method.[50]
Result
positive after 1 week to 4 months
ECG
Test
Should be performed in all patients owing to associated arrhythmias secondary to myocarditis. Cardiac monitoring is also recommended during treatment.
Result
atrial fibrillation; atrial flutter; tachycardia; premature ventricular contractions or ventricular tachycardia
chest x-ray
LFTs
Test
Should be ordered in all patients in the immune phase.
Result
elevated aminotransferases and/or alkaline phosphatase
conjugated bilirubin
Test
Should be ordered in all patients in the immune phase.
Result
elevated direct bilirubin; markedly elevated conjugated bilirubin levels (≤80 mg/dL)
metabolic profile
Test
Should be ordered in all patients in the immune phase.
Result
elevated BUN and creatinine; hypokalemia
serum pancreatic enzymes
Test
A small proportion of patients develop acute pancreatitis as a complication, which can be fatal.[8]
Result
amylase and lipase may be elevated
CSF analysis
Test
Should be ordered in all patients in the immune phase. Indicates aseptic meningitis.
Result
cell counts below 500/mm³ with lymphocytic pleocytosis; elevated protein; normal glucose
Tests to consider
urine culture
Test
May be ordered in the immune phase.
Result
positive after 1 week to 4 months if collected during second week of disease
renal biopsy
Test
Diagnostic for acute interstitial nephritis, immune-complex glomerulonephritis. Usually performed during the immune phase and recommended in patients with renal involvement in order to document the type of kidney injury.
Result
findings include tubulointerstitial inflammatory cell infiltrate of lymphocytes; plasma cells; macrophages; and polymorphonuclear infiltrates with focal areas of tubular necrosis
lung biopsy
staining methods
Test
Includes silver staining, immunoperoxidase staining, and immunofluorescent staining. These staining methods are not widely used.[Figure caption and citation for the preceding image starts]: Silver stain on liver biopsy showing leptospiresImage provided by the CDC and the Public Health Image Library [Citation ends].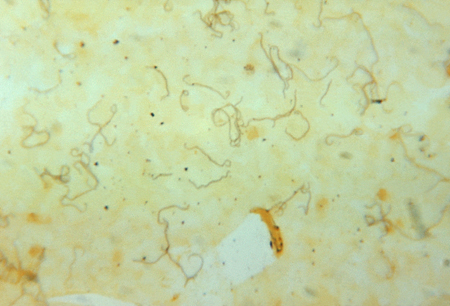
Result
identifies presence of spirochete in tissue
latex agglutination
Test
Shown to be sensitive and specific.[62]
Result
positive
western blot
Test
Shown to be sensitive and specific.[62]
Result
positive
quantitative PCR
Test
Has been evaluated as an aid to provide an accurate and fast diagnosis in patients presenting with clinical manifestations suggestive of leptospirosis in endemic areas.[63]
Some studies have found that leptospiremia levels measured by quantitative PCR are associated with disease severity when obtained early in infection; this may be a valuable method to predict clinical course.[44]
Result
positive
Emerging tests
lateral flow assays
Test
While not yet widely employed, lateral flow assays are a promising diagnostic modality, although there is considerable variability in published data regarding their sensitivity (55% to 93%) and specificity (57% to 99%).[64] Several factors may account for this variability (including variations in reference tests and the stage of infection when the testing was performed, with a lower sensitivity described in the first week of infection).[64]
Result
positive
cytokines
Test
Current evidence suggests that interleukin (IL)-1b, IL-2, IL-4, IL-6, IL-8, IL-10, and tumor necrosis factor (TNF)-alpha levels are higher in severe cases of leptospirosis in comparison with mild cases.[65] The day of infection appears to be an important determinant of cytokine level; further studies are needed before cytokine levels can be used to monitor infection.[65][66]
Result
higher levels may indicate severe infection
Use of this content is subject to our disclaimer