Tests
1st tests to order
CBC with differential
Test
The CBC may show pancytopenia (decreased cell count in all three cell lines), which is characteristic of classic HCL.[6][35]
The majority of patients with classic HCL present with leukopenia.[7][43] However, in approximately 10% of patients, leukocytosis (WBC count >10,000 to 20,000/microliter) is present.[7][43] Hairy cells are the predominant circulating WBC in patients presenting with leukocytosis.
Neutropenia and monocytopenia are generally present.[7][35] Monocytopenia is a consistent finding (present in approximately 90% of patients) and is characteristic of classic HCL.[7][36][44] Some automated hematology analyzers may classify hairy cells as monocytes, which can mask monocytopenia unless peripheral blood is examined.[45]
Result
may show pancytopenia; isolated or combination of leukopenia (neutropenia, monocytopenia), anemia, and/or thrombocytopenia; leukocytosis (WBC count >10,000-20,000/microliter) occurs in approximately 10% to 20% of patients
peripheral blood smear
bone marrow trephine biopsy and aspiration (morphology assessment)
Test
To confirm the diagnosis of HCL, a bone marrow trephine biopsy and aspiration should be carried out for morphology assessment and immunophenotyping (using immunohistochemistry or flow cytometry).[7][34]
Assessment of the bone marrow specimen will show a pattern of hairy cell infiltration with a single round or oval nucleus separated by abundant cytoplasm in a fine fibrillar network. The cell appears separated, resulting in the characteristic fried egg appearance.
Staining of the bone marrow smear for reticulin will reveal the presence of reticulin fibers, which appear to surround individual hairy cells.[45]
Hypocellular bone marrow is present in approximately 10% of patients; avoiding a misdiagnosis of aplastic anemia is important in these patients.[33]
Bone marrow aspiration is often difficult to carry out in patients with classic HCL and usually results in a dry tap (due to bone marrow fibrosis).
[Figure caption and citation for the preceding image starts]: Cytospin prepared from bone marrow aspirate illustrates the typical cell cytology, with oval- to bean-shaped nuclei and moderate amounts of cytoplasm with irregular cytoplasmic borders (Wright Giemsa 100×oil)From the collection of Lynn Moscinski, MD [Citation ends].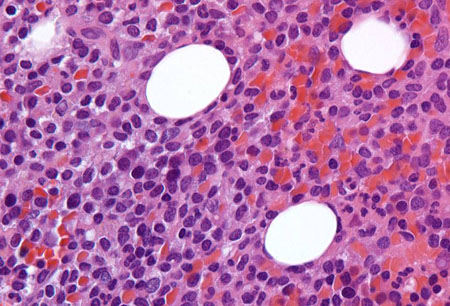 [Figure caption and citation for the preceding image starts]: Sections of core biopsy demonstrate lymphocytes with obvious cytoplasm within the marrow interstitium, associated with dilation of marrow sinuses and red blood cell collections (H&E 50×oil)From the collection of Lynn Moscinski, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Sections of core biopsy demonstrate lymphocytes with obvious cytoplasm within the marrow interstitium, associated with dilation of marrow sinuses and red blood cell collections (H&E 50×oil)From the collection of Lynn Moscinski, MD [Citation ends].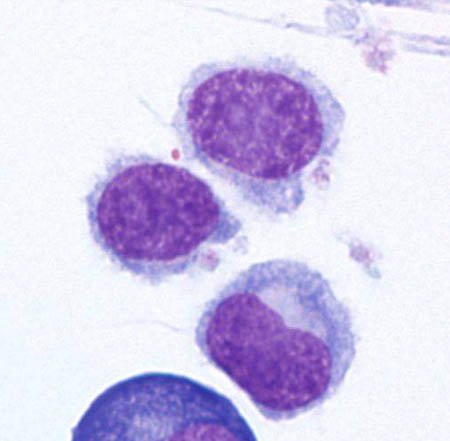
Result
presence of hairy cells in the bone marrow; presence of reticulin fibrosis; hypocellular bone marrow (uncommon)
immunophenotyping (immunohistochemistry or flow cytometry)
Test
Immunohistochemistry (using bone marrow biopsy specimen) or flow cytometry (using bone marrow aspirate or peripheral blood) can help differentiate classic HCL from other lymphoproliferative disorders (including HCL variant [HCL-V]; also known as splenic B-cell lymphoma/leukemia with prominent nucleoli [SBLPN]), and is important for establishing the diagnosis.[7][34]
Immunophenotyping should test for CD19, CD20, CD5, CD10, CD11c, CD22, CD25, CD103, CD123, cyclin D1, CD200, and annexin A1 (ANXA1).
ANXA1 appears to be a specific marker for differential diagnosis because no other B-cell lymphoma seems to express it.[41] However, it is not useful for detection of minimal residual disease.[7]
HCL cells do not express CD21, a marker for immature B cells.
Immunohistochemistry may also test for tartrate-resistant acid phosphatase (TRAP), which is expressed on HCL cells.[23][46]
Result
positive for immunophenotypic markers for HCL
comprehensive metabolic panel
Test
Includes urea, serum creatinine, electrolytes, serum albumin, and liver function tests (LFTs).
Can guide treatment and should be ordered for pretreatment evaluation.[37]
Assessment of renal function is important if treatment with a purine analog is planned.
Result
may be normal or abnormal
serum lactate dehydrogenase (LDH)
Test
Can guide treatment and should be ordered for pretreatment evaluation.[37]
Result
may be normal or abnormal
viral serology for hepatitis B and C
Test
Can guide treatment and should be ordered for pretreatment evaluation.[37]
Treatments for HCL may increase the risk for reactivation.
Result
may be positive
Tests to consider
molecular analysis (for BRAF V600E mutation or IGHV4-34 rearrangement)
Test
Molecular analysis may be considered to detect the BRAF V600E mutation (if there is diagnostic uncertainty following immunophenotyping) and IGHV4-34 rearrangements.[7][34]
The BRAF V600E mutation is present in almost all patients with classic HCL, but absent in HCL variant (HCL-V; also known as splenic B-cell lymphoma/leukemia with prominent nucleoli [SBLPN]).[27]
Patients with IGHV4-34 mutant HCL do not respond well to purine analogs and have a poor prognosis. The BRAF V600E mutation is usually absent in these patients.[47]
Result
positive for BRAF V600E mutation, or may be positive for IGHV4-34 rearrangement
CT chest, abdomen, and pelvis
Test
Imaging is not required except in milder forms of disease, in which CT scans of the chest, abdomen, and pelvis may be used to detect mild organomegaly and adenopathy.[34][37][48]
CT can detect internal adenopathy in approximately 15% of patients.[48]
Result
may show splenomegaly, hepatomegaly, lymphadenopathy
Use of this content is subject to our disclaimer