Diagnosis is made by assessing signs and symptoms, biochemical evidence of hyperthyroidism, and radioisotope scan with typical uptake and appearance.
History and physical
History of living in an iodine-deficient region should be sought. Onset of symptoms for toxic multinodular goiter (MNG) is more insidious and the symptoms less dramatic than for Graves disease.[11]Krohn K, Führer D, Bayer Y, et al. Molecular pathogenesis of euthyroid and toxic multinodular goiter. Endocr Rev. 2005;26:504-24.
https://academic.oup.com/edrv/article/26/4/504/2355182?login=true
http://www.ncbi.nlm.nih.gov/pubmed/15615818?tool=bestpractice.com
Younger patients are more likely to have typical symptoms of hyperthyroidism, such as hyperphagia, weight loss, sweating, heat intolerance, nervousness, palpitations, oligomenorrhea, or hyperdefecation.
Older patients may have apathetic hyperthyroidism with mood change, weight loss, or atrial fibrillation alone.[5]Thiruvengadam S, Luthra P. Thyroid disorders in elderly: A comprehensive review. Dis Mon. 2021 Nov;67(11):101223.
https://www.doi.org/10.1016/j.disamonth.2021.101223
http://www.ncbi.nlm.nih.gov/pubmed/34154807?tool=bestpractice.com
The conduction system is slower in older people than in young people; therefore, tachycardia is less common and the ventricular rate in atrial fibrillation may not be rapid.
A goiter is usually present but can be small or nonpalpable, particularly in older patients. Some patients present with symptoms of neck compression such as dysphagia, dyspnea, or a choking sensation, but other causes need to be ruled out.[1]Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract. 2016 May;22(5):622-39.
https://www.endocrinepractice.org/article/S1530-891X(20)42954-4/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/27167915?tool=bestpractice.com
In severe cases of thoracic inlet obstruction, a Pemberton sign may be present (extension of arms over the head results in jugular venous distension and facial plethora).[22]Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;26:348:2646-2655. [Erratum in: N Engl J Med. 2003;349:620.]
http://www.ncbi.nlm.nih.gov/pubmed/12826640?tool=bestpractice.com
[23]De Filippis EA, Sabet A, Sun MR, et al. Pemberton's sign: explained nearly 70 years later. J Clin Endocrinol Metab. 2014;99:1949-1954.
http://www.ncbi.nlm.nih.gov/pubmed/24646105?tool=bestpractice.com
Physical findings may include warm moist skin, stare, lid lag, tremor, or proximal muscle weakness when hyperthyroidism is overt. Stigmata of Graves disease, including exophthalmos and pretibial myxedema, are absent.[3]De Leo S, Lee SY, Braverman LE. Hyperthyroidism. Lancet. 2016 Aug 27;388(10047):906-18.
http://www.ncbi.nlm.nih.gov/pubmed/27038492?tool=bestpractice.com
Tests
Thyroid-stimulating hormone (TSH) is the initial screening test.[13]Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26:1343-1421.
http://online.liebertpub.com/doi/10.1089/thy.2016.0229
http://www.ncbi.nlm.nih.gov/pubmed/27521067?tool=bestpractice.com
[24]National Institute for Health and Care Excellence. Thyroid disease: assessment and management. Oct 2023 [internet publication].
https://www.nice.org.uk/guidance/ng145
Do not order more tests until the results of the TSH test are available as a TSH value within the reference range excludes the majority of primary thyroid diseases.[25]American Society for Clinical Pathology. Thirty five things physicians and patients should question. Choosing Wisely, an initiative of the ABIM Foundation. Jul 2021 [internet publication].
https://web.archive.org/web/20230316185857/https://www.choosingwisely.org/societies/american-society-for-clinical-pathology
If TSH is suppressed, thyroid hormone levels (T4/T3) should be measured. The preferred tests are: free T4; and total T3 plus a measure of binding. Generally, free T4 level is elevated. Some patients may have subclinical hyperthyroidism with suppressed TSH and normal levels of thyroid hormones. T3 is elevated and T4 is usually high-normal in T3 toxicosis.[13]Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26:1343-1421.
http://online.liebertpub.com/doi/10.1089/thy.2016.0229
http://www.ncbi.nlm.nih.gov/pubmed/27521067?tool=bestpractice.com
[24]National Institute for Health and Care Excellence. Thyroid disease: assessment and management. Oct 2023 [internet publication].
https://www.nice.org.uk/guidance/ng145
In the absence of stigmata of Graves disease or positive TSH receptor antibodies, thyroid scan and uptake are indicated when biochemical hyperthyroidism is confirmed. In toxic MNG, this shows multiple hot and cold areas consistent with areas of autonomy and suppression. I-123 is the preferred isotope.[26]American College of Radiology. ACR Appropriateness Criteria®. Thyroid disease. 2018 [internet publication].
https://acsearch.acr.org/docs/3102386/narrative
Tc-99 pertechnetate scan is an alternative for imaging the thyroid, but there is a risk of false-positive images and uptake cannot be measured.[1]Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract. 2016 May;22(5):622-39.
https://www.endocrinepractice.org/article/S1530-891X(20)42954-4/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/27167915?tool=bestpractice.com
I-123 uptake is typically lower than for Graves disease and is often within the normal range.
Thyroid ultrasound is not helpful for diagnosis, but may be used to further define any cold nodules found on scan. Cold nodules >1 cm in diameter with suspicious ultrasonographic characteristics (such as more-tall-than-wide shape, irregular margins, microcalcifications, or marked hypoechogenicity) should be considered for further evaluation with fine needle biopsy.[1]Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract. 2016 May;22(5):622-39.
https://www.endocrinepractice.org/article/S1530-891X(20)42954-4/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/27167915?tool=bestpractice.com
[27]Singh Ospina N, Iñiguez-Ariza NM, Castro MR. Thyroid nodules: diagnostic evaluation based on thyroid cancer risk assessment. BMJ. 2020 Jan 7;368:l6670.
https://www.doi.org/10.1136/bmj.l6670
http://www.ncbi.nlm.nih.gov/pubmed/31911452?tool=bestpractice.com
[28]Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1-133.
http://online.liebertpub.com/doi/pdf/10.1089/thy.2015.0020
http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com
[29]Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid. 2017 Nov;27(11):1341-6.
https://www.liebertpub.com/doi/10.1089/thy.2017.0500
http://www.ncbi.nlm.nih.gov/pubmed/29091573?tool=bestpractice.com
CBC may show nonspecific anemia or leukocytosis. Baseline WBC count is useful prior to starting antithyroid drugs. Mild neutropenia should not be regarded as a contraindication to the use of antithyroid drug therapy and hyperthyroidism typically normalizes the neutrophil count.[30]Scappaticcio L, Maiorino MI, Maio A, et al. Neutropenia in patients with hyperthyroidism: systematic review and meta-analysis. Clin Endocrinol (Oxf). 2021 Mar;94(3):473-83.
https://www.doi.org/10.1111/cen.14313
http://www.ncbi.nlm.nih.gov/pubmed/32799342?tool=bestpractice.com
Blood chemistries may show elevated LFTs or calcium. Elevated alkaline phosphatase is generally of bony origin, due to increased bone turnover. Most patients with hyperthyroidism will have elevated transaminases prior to initiating treatment and levels typically improve with antithyroid drug therapy.[31]Scappaticcio L, Longo M, Maiorino MI, et al. Abnormal liver blood tests in patients with hyperthyroidism: systematic review and meta-analysis. Thyroid. 2021 Jun;31(6):884-94.
https://www.doi.org/10.1089/thy.2020.0715
http://www.ncbi.nlm.nih.gov/pubmed/33327837?tool=bestpractice.com
Thyroid peroxidase antibodies are nonspecific, but a positive result may support a diagnosis of Graves disease. TSH receptor antibodies may be useful to distinguish toxic MNG from Graves disease; third-generation TSH receptor antibody assays are highly sensitive and specific for Graves disease.
An ECG may be required for suspected dysrhythmia. Occasionally a noncontrast CT scan of the neck is indicated to evaluate a large goiter with compressive symptoms, or as part of a preoperative evaluation before thyroidectomy. [Figure caption and citation for the preceding image starts]: Thyroid scan showing variegated uptake in toxic multinodular goiterCourtesy of Dr Elizabeth Pearce; used with permission [Citation ends].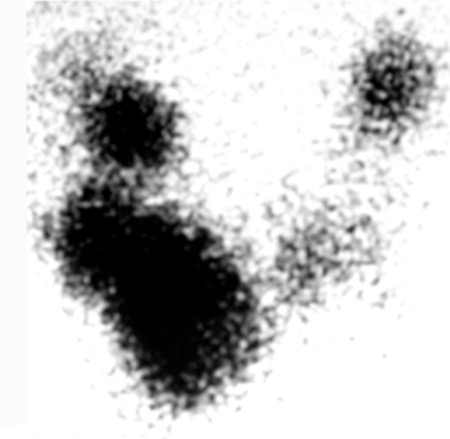 [Figure caption and citation for the preceding image starts]: Chest CT showing marked enlargement of the thyroid gland with an extensive intrathoracic component causing trachea compressionDias T et al. Acute airway obstruction due to benign multinodular goitre. BMJ Case Reports. 2019;12:e228095; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Chest CT showing marked enlargement of the thyroid gland with an extensive intrathoracic component causing trachea compressionDias T et al. Acute airway obstruction due to benign multinodular goitre. BMJ Case Reports. 2019;12:e228095; used with permission [Citation ends].