History
Most studies of head lice, both in the US and in other industrialized countries, report the highest incidence in elementary school-aged children (3-12 years of age).[12]Burgess I. Human lice and their control. Ann Rev Entomol. 2004 Jan;49:457-81.
http://www.ncbi.nlm.nih.gov/pubmed/14651472?tool=bestpractice.com
[6]Downs A, Oxley J. Head lice infestations in different ethnic groups. Int J Derm. 2001 Mar;40(3):237-8.
http://www.ncbi.nlm.nih.gov/pubmed/11422534?tool=bestpractice.com
[15]Gratz NG; World Health Organization/WHOPES. Human lice: their prevalence, control and resistance to insecticides - a review, 1985-1997. August 1997 [internet publication].
https://apps.who.int/iris/bitstream/handle/10665/63791/WHO_CTD_WHOPES_97.8.pdf
Lice do not hop or jump, they can only crawl, so adults with head lice are most likely to be parents of children with lice, or those living in overcrowded conditions.[5]American Academy of Pediatrics, Nolt D, Moore S, et al. Head Lice. Pediatrics. 2022 Oct 1;150(4):e2022059282.
https://publications.aap.org/pediatrics/article/150/4/e2022059282/189566/Head-Lice
http://www.ncbi.nlm.nih.gov/pubmed/36156158?tool=bestpractice.com
Indirect transmission through contact with personal belongings is much less likely to occur. Most studies that report incidence of head lice infestation by gender in school-aged children indicate about a 2 to 3:1 female-to-male ratio.[12]Burgess I. Human lice and their control. Ann Rev Entomol. 2004 Jan;49:457-81.
http://www.ncbi.nlm.nih.gov/pubmed/14651472?tool=bestpractice.com
[15]Gratz NG; World Health Organization/WHOPES. Human lice: their prevalence, control and resistance to insecticides - a review, 1985-1997. August 1997 [internet publication].
https://apps.who.int/iris/bitstream/handle/10665/63791/WHO_CTD_WHOPES_97.8.pdf
[22]Estrada JS, Morris RI. Pediculosis in a school population. J Sch Nurs. 2000 Aug;16(3):32-8.
http://www.ncbi.nlm.nih.gov/pubmed/11885087?tool=bestpractice.com
Other key risk factors include race other than black, overcrowding or close living conditions (e.g., sleepovers or camp in the preceding month, boarding school), and close contact with an infected individual.[12]Burgess I. Human lice and their control. Ann Rev Entomol. 2004 Jan;49:457-81.
http://www.ncbi.nlm.nih.gov/pubmed/14651472?tool=bestpractice.com
[6]Downs A, Oxley J. Head lice infestations in different ethnic groups. Int J Derm. 2001 Mar;40(3):237-8.
http://www.ncbi.nlm.nih.gov/pubmed/11422534?tool=bestpractice.com
[15]Gratz NG; World Health Organization/WHOPES. Human lice: their prevalence, control and resistance to insecticides - a review, 1985-1997. August 1997 [internet publication].
https://apps.who.int/iris/bitstream/handle/10665/63791/WHO_CTD_WHOPES_97.8.pdf
Lice spread most readily through head-to-head contact. Any situation that brings infested children in close contact with others is very likely to cause spread of that infestation.[24]Chunge RN, Scott FE, Underwood JE, et al. A pilot study to investigate transmission of head lice. Can J Public Health. 1991 May-Jun;82(3):207-8.
http://www.ncbi.nlm.nih.gov/pubmed/1884317?tool=bestpractice.com
[27]Burkhart CN, Burkhart CG. Fomite transmission in head lice. J Am Acad Derm. 2007 Jun;56(6):1044-7.
http://www.ncbi.nlm.nih.gov/pubmed/17187895?tool=bestpractice.com
[31]American Academy of Pediatrics. Head lice. In: 2006 Red Book: report of the committee on infectious diseases. 27:448-92. Therefore, having a family member or bedmate with head lice greatly increases the risk.[24]Chunge RN, Scott FE, Underwood JE, et al. A pilot study to investigate transmission of head lice. Can J Public Health. 1991 May-Jun;82(3):207-8.
http://www.ncbi.nlm.nih.gov/pubmed/1884317?tool=bestpractice.com
Generally, a parent or teacher will observe excessive scalp scratching in the child, or a child may complain of a pruritic scalp.
Physical examination
People who are suspected of having head lice, including those who have been in close contact with an individual with head lice, should have a careful scalp examination, even in the absence of symptoms. Also, anyone who is noted to have a scalp infection (e.g., impetigo or pyoderma) or otherwise unexplained lymphadenopathy in the head or neck region should be carefully checked for the presence of head lice infestation.[12]Burgess I. Human lice and their control. Ann Rev Entomol. 2004 Jan;49:457-81.
http://www.ncbi.nlm.nih.gov/pubmed/14651472?tool=bestpractice.com
[3]Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004 Jan;50(1):1-12.
http://www.ncbi.nlm.nih.gov/pubmed/14699358?tool=bestpractice.com
[4]Leung AK, Fong JH, Pinto-Rojas A. Pediculosis capitis. J Ped Health Care. 2005 Nov-Dec;19(6):369-73.
http://www.ncbi.nlm.nih.gov/pubmed/16286223?tool=bestpractice.com
The definitive standard for diagnosis is finding a live louse or lice on the head.[1]Burgess IF, Silverston P. Head lice. Clin Evid (Online). January 2015 [internet publication].
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4294162
http://www.ncbi.nlm.nih.gov/pubmed/25587918?tool=bestpractice.com
[5]American Academy of Pediatrics, Nolt D, Moore S, et al. Head Lice. Pediatrics. 2022 Oct 1;150(4):e2022059282.
https://publications.aap.org/pediatrics/article/150/4/e2022059282/189566/Head-Lice
http://www.ncbi.nlm.nih.gov/pubmed/36156158?tool=bestpractice.com
[35]Pollack RJ, Kiszewski AD, Spielman A. Overdiagnosis and consequent mismanagement of head louse infestation in North America. Pediatr Infect Dis J. 2000 Aug;19(8):689-93.
http://www.ncbi.nlm.nih.gov/pubmed/10959734?tool=bestpractice.com
This can be difficult to do, because lice tend to crawl quickly. The child should be positioned with his or her head tilted to the chest and the hair closest to the nape of the neck and behind the ears examined under good light, separating the hair into segments with fingers, sticks/throat culture swabs, or tongue depressors.
Combing is more accurate than visual inspection at diagnosing infestation. Visual inspection has been reported to underestimate the true prevalence of active infestation by a factor of 3.5, although visual inspection has a higher sensitivity for the diagnosis of historic infestation.[36]Jahnke C, Bauer E, Hengge UR, et al. Accuracy of diagnosis of pediculosis capitis: visual inspection vs wet combing. Arch Dermatol. 2009 Mar;145(3):309-13.
http://archderm.jamanetwork.com/article.aspx?articleid=711918
http://www.ncbi.nlm.nih.gov/pubmed/19289764?tool=bestpractice.com
The hair is moistened with water (to make it easier for lice to stick to the comb) or conditioner (to slow the lice and make combing easier). The moistened hair should be combed with a fine-toothed nit comb, especially near the nape of the neck and behind the ears, checking for nymphs or adult lice. Dry combing can produce false-negative results because the lice are apt to crawl away quickly from the site being combed. In addition, dry combing should be undertaken with caution, as vigorous combing with a plastic comb can generate enough static electricity to eject lice, which can then set up an infestation elsewhere, depending on where they land.[29]Williams LK, Reichert A, MacKenzie WR, et al. Lice, nits, and school policy. Pediatrics. 2001 May;107(5):1011-5.
http://www.ncbi.nlm.nih.gov/pubmed/11331679?tool=bestpractice.com
[31]American Academy of Pediatrics. Head lice. In: 2006 Red Book: report of the committee on infectious diseases. 27:448-92.[32]Public Health Medicine Environmental Group. Head lice: evidence-based guidelines based on the Stafford Report - 2012 update [internet publication].
https://www.nhsggc.org.uk/media/239960/stafford-head-lice-2012.pdf
[33]Mumcuoglu KY, Friger M, Ioffe-Uspensky I, et al. Louse comb versus direct visual examination for the diagnosis of head louse infestations. Ped Derm. 2001 Jan-Feb;18(1):9-12.
http://www.ncbi.nlm.nih.gov/pubmed/11207962?tool=bestpractice.com
[34]Burgess I. Detection combing. Nurs Times. 2002 Nov 12-18;98(46):57.
http://www.ncbi.nlm.nih.gov/pubmed/12478939?tool=bestpractice.com
[37]Balcioglu C, Burgess IF, Limoncu ME, et al. Plastic detection comb better than visual screening for diagnosis of head louse infestation. Epidemiol Infect. 2008 Oct;136(10):1425-31.
http://www.ncbi.nlm.nih.gov/pubmed/18177517?tool=bestpractice.com
Some will accept the presence of live eggs within 1 cm of the scalp as a diagnosis of head lice infestation, but several investigators have shown that many patients with eggs alone never "convert" to an active infestation.[29]Williams LK, Reichert A, MacKenzie WR, et al. Lice, nits, and school policy. Pediatrics. 2001 May;107(5):1011-5.
http://www.ncbi.nlm.nih.gov/pubmed/11331679?tool=bestpractice.com
[35]Pollack RJ, Kiszewski AD, Spielman A. Overdiagnosis and consequent mismanagement of head louse infestation in North America. Pediatr Infect Dis J. 2000 Aug;19(8):689-93.
http://www.ncbi.nlm.nih.gov/pubmed/10959734?tool=bestpractice.com
[38]Hootman J. Quality improvement projects related to pediculosis management. J School Nursing. 2002 Apr;18(2):80-6.
http://www.ncbi.nlm.nih.gov/pubmed/12017250?tool=bestpractice.com
Finding empty egg cases (nits) >1 cm from the scalp should not be accepted as a diagnosis of a lice infestation.
Although not always seen, tiny papules at the nape of the neck just below the hairline are not uncommon, and represent louse bites. Surrounding inflammation is secondary to the body's reaction to the louse saliva.[13]Meinking TL. Infestations: pediculosis. Curr Probl Dermatol. 1996;24:157-63.
http://www.ncbi.nlm.nih.gov/pubmed/8743266?tool=bestpractice.com
Lice very rarely leave a head, but can occasionally be seen on the collar area of clothing in an unusually severe infestation. Lice discovered on the collar area of clothing could either be head lice (most likely diagnosis for a child) or body lice (if the person is homeless or destitute).[35]Pollack RJ, Kiszewski AD, Spielman A. Overdiagnosis and consequent mismanagement of head louse infestation in North America. Pediatr Infect Dis J. 2000 Aug;19(8):689-93.
http://www.ncbi.nlm.nih.gov/pubmed/10959734?tool=bestpractice.com
Examination with magnifying lens, trichoscope or microscope
In cases where the diagnosis is in question, examination with a magnifying lens, trichoscope, or microscope can distinguish between a nymph or adult louse and other insects or hair debris. An egg with an eye spot can be distinguished from an empty egg case, or nit. A nit can be distinguished from dandruff or other hair debris, which can sometimes be difficult to distinguish on casual observation with the naked eye. Nits are firmly attached to the hair shaft, and can be removed using fingernails or a fine-toothed lice comb. An alternative is plucking the hair with the nit, and examining that under the microscope.
Because school nurses rarely have these devices available, a referral to the health care provider's office may be required.[35]Pollack RJ, Kiszewski AD, Spielman A. Overdiagnosis and consequent mismanagement of head louse infestation in North America. Pediatr Infect Dis J. 2000 Aug;19(8):689-93.
http://www.ncbi.nlm.nih.gov/pubmed/10959734?tool=bestpractice.com
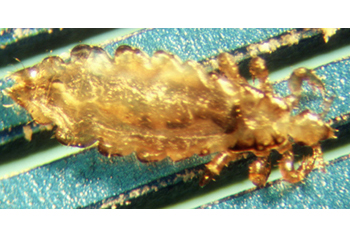
[Figure caption and citation for the preceding image starts]: Adult louse seen under a microscopeFrom the collection of Dr Richard Pollack; used with permission [Citation ends].