Approach
Testing is not routine, and diagnosis is based primarily on the clinical appearance.[Figure caption and citation for the preceding image starts]: Seborrheic keratosis on the chest of an elderly womanFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Seborrheic keratosis of the chest: clinical overview imageFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Seborrheic keratosis of the chest: clinical overview imageFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Seborrheic keratosis of the chest: clinical close-up imageFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Seborrheic keratosis of the chest: clinical close-up imageFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Dermoscopic image of seborrheic keratosis on the chestFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermoscopic image of seborrheic keratosis on the chestFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Clinical close-up image of seborrheic keratosis on the back of a 40-year-old manFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Clinical close-up image of seborrheic keratosis on the back of a 40-year-old manFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Clinical overview image of seborrheic keratosis on the back of a 40-year-old manFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Clinical overview image of seborrheic keratosis on the back of a 40-year-old manFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Clinical image of an example of a dark-brown pigmented seborrheic keratosisFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Clinical image of an example of a dark-brown pigmented seborrheic keratosisFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Example of a dark-brown pigmented seborrheic keratosis. Dermoscopic image: see yellowish horn pearls and dark brown holes corresponding to so-called "pseudo-follicular openings"From the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Example of a dark-brown pigmented seborrheic keratosis. Dermoscopic image: see yellowish horn pearls and dark brown holes corresponding to so-called "pseudo-follicular openings"From the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].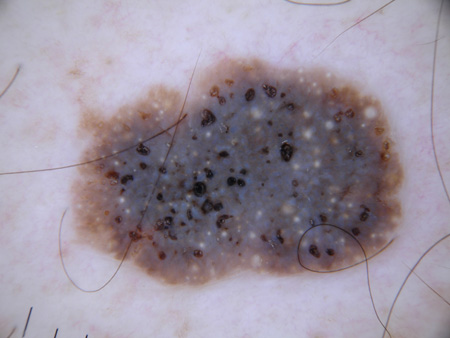
Clinical appearance
The clinical criteria used for the diagnosis of seborrheic keratosis are based on the location and appearance of the lesions. Lesions generally occur in multiples rather than as single lesions. They are more frequently found on the torso and chest, then the temple, scalp, and neck. They can occur on any part of the body except mucous membranes.
Lesions can display a variety of colors, but are usually yellow or light-to-dark brown. The classic appearance is that they look "stuck on". They have a slightly raised, flat surface and a wart-like texture. On the surface of the lesions, round yellow-white horn pearls can be visible.
Lesions are painless, although they can itch and become inflamed, either through friction with clothing or spontaneously.
Dermoscopic features
The diagnosis of seborrheic keratosis is generally made clinically. Dermoscopy is being increasingly used in primary and secondary care to differentiate between benign and malignant pigmented lesions. UK National Institute of Health and Care Excellence (NICE) guidance recommends that any patient undergoing a specialist assessment for pigmented lesions must be examined with a dermatoscope.[20]
Machine-learning algorithms are being investigated for the purposes of pigmented skin lesion classification (including diagnosis of seborrheic keratoses) and early studies are promising but this modality is not being used in clinical practice yet.[21]
The characteristic dermoscopic features of seborrheic keratosis are milia-like cysts and comedo-like openings. Milia-like cysts are white or yellowish round structures that correspond to small intraepidermal, keratin-filled cysts (horn pearls). They are not exclusively found in seborrheic keratosis as they are also seen in congenital nevi and papillomatous dermal nevi, but less frequently.
Comedo-like openings (also known as pseudofollicular openings or crypts) are brownish holes in the surface of seborrheic keratosis that correspond histologically to keratin-filled invaginations of the epidermis.[22][23][24] Further dermoscopic criteria include a gyrated surface (brain-like-appearance) and looped vessels.[Figure caption and citation for the preceding image starts]: Dermoscopic image of seborrheic keratosis on the chestFrom the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Example of a dark-brown pigmented seborrheic keratosis. Dermoscopic image: see yellowish horn pearls and dark brown holes corresponding to so-called "pseudo-follicular openings"From the collection of Dr Braun and Dr Kolm, used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Typical dermoscopic appearance of seborrheic keratosis with milia-like cysts (black arrows) and comedo-like openings (blue arrows)Primary Care Dermatology Society (PCDS); used with permission [Citation ends].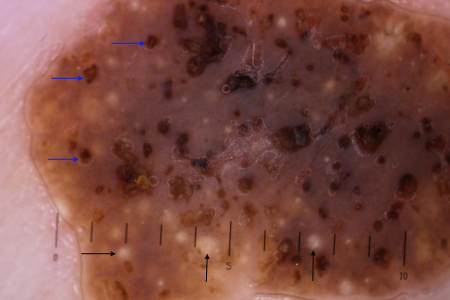
Reflectance confocal microscopy
As the clinical and dermoscopic examination of irritated, regressive, or highly pigmented seborrheic keratosis may show features associated with malignant skin tumors (e.g., malignant melanoma, basal cell carcinoma) reflectance confocal microscopy (RCM) may be added as an additional tool for diagnosis. RCM is a noninvasive imaging method that allows the in vivo examination of skin at cellular-level resolution. RCM features that indicate the diagnosis of seborrheic keratosis are: cerebriform surface structures; keratin-filled invaginations; corneal pseudocysts; a regular honeycomb pattern at epidermal layers; cords and polymorphous papillae at the dermo-epidermal junction; melanophages and looped vessels at the papillary dermis; and the absence of RCM features suggestive of malignancy.[25]
Biopsy
A biopsy of a lesion may be used to confirm diagnosis, especially in lesions that itch or bleed, become inflamed and red, and are of dark brown to black color. Biopsy is recommended in any isolated dark seborrheic keratosis.
Use of this content is subject to our disclaimer