Tests
1st tests to order
culture and Gram stain
Test
Gold standard test for diagnosis. Should be ordered in all patients with suspected anthrax.
The specimen collected for testing depends on the clinical presentation.[49]
Cutaneous anthrax: lesion swabs are recommended by the Centers for Disease Control and Prevention (CDC). Sensitivity is limited (60% to 65%).[52] Blood cultures are only recommended in patients with signs of systemic infection (e.g., fever, tachycardia, tachypnea, hypotension).
Inhalation anthrax: blood and pleural fluid are recommended by the CDC.
Ingestion anthrax: blood and ascites fluid are recommended by the CDC. A rectal swab may be collected in patients with gastrointestinal infection, or an oropharyngeal swab in patients with oropharyngeal infection.
Injection anthrax: blood is recommended by the CDC.
Anthrax meningitis: blood and cerebrospinal fluid (CSF) should be tested in patients with signs of meningitis (e.g., severe headache, meningeal signs, altered mental status, seizures).
Result
gram-positive bacilli in short chains; flat, nonhemolytic mucoid colonies on 5% sheep's blood agar; neutrophilic pleocytosis (CSF)
real-time polymerase chain reaction (RT-PCR)
Test
The specimen collected for testing depends on the clinical presentation.[49]
Cutaneous anthrax: lesion swabs are recommended by the CDC.
Inhalation anthrax: blood and pleural fluid are recommended by the CDC.
Ingestion anthrax: blood and ascites fluid are recommended by the CDC. A rectal swab may be collected in patients with gastrointestinal infection, or an oropharyngeal swab in patients with oropharyngeal infection.
Injection anthrax: blood is recommended by the CDC.
Anthrax meningitis: blood and CSF should be tested in patients with signs of meningitis (e.g., severe headache, meningeal signs, altered mental status, seizures).
Result
positive for Bacillus anthracis or anthrax toxin genes
serology
Test
Acute (i.e., ≤7 days after symptom onset or as soon as possible after a known exposure) and convalescent (14-35 days after symptom onset) serum samples should be taken in all patients, regardless of the anthrax subtype.[49]
Result
four-fold rise in antibodies to protective antigen between acute and convalescent sera; four-fold change in antibodies to protective antigen in paired convalescent sera using CDC quantitative anti-PA immunoglobulin G (IgG) enzyme-linked immunosorbent assay (ELISA) testing in an unvaccinated person
anthrax lethal factor (LF) toxin mass spectrometry
Test
Serum or plasma samples should be collected for LF testing in all patients, regardless of the anthrax subtype. Plasma is the preferred specimen. Pleural fluid may be used in patients with inhalation anthrax, and ascites fluid may be used in patients with ingestion anthrax.[49]
Result
detection of anthrax lethal factor toxin
biopsy
Test
Biopsy specimens depend on the clinical presentation.[49]
Cutaneous anthrax: a punch biopsy of a papule or vesicle for histopathology and immunohistochemistry (IHC) is an alternative test when cutaneous anthrax is suspected and wound cultures are negative or cannot be obtained due to a paucity of fluid.[37][53]
Inhalation anthrax: pleural and/or bronchial biopsies may be collected for IHC.
Injection anthrax: tissue biopsy from localized lesion tissue debridement.
Result
necrosis of the dermis and epidermis, edema, and mild inflammatory infiltrate on hematoxylin and eosin stain (cutaneous anthrax); detection of B anthracis antigens in tissues by immunohistochemical staining using both B anthracis cell wall and capsule monoclonal antibodies
CBC
Test
If inhalation anthrax is suspected, a white blood cell count should be obtained and tracked.[51]
Result
elevated white blood cell count
chest x-ray
Test
In all suspected cases of inhalation or systemic B anthracis infection, a chest x-ray should be ordered.
Findings are not specific but are sensitive.[37][54] In the anthrax attacks of 2001, pleural effusions and widened mediastinum were noted in 70% to 80% of cases.[51][Figure caption and citation for the preceding image starts]: Chest x-ray findings of inhalation anthraxBorio et al. JAMA 2001;286:2554-2559 [Citation ends].
Result
widened mediastinum, hilar and mediastinal fullness suggestive of lymphadenopathy, and large pleural effusions
Tests to consider
CT chest
Test
If the chest x-ray is normal in suspected cases of inhalation anthrax, chest CT is recommended.[51][55][56][57][Figure caption and citation for the preceding image starts]: Chest CT reveals perihilar lymphadenopathy, perihilar infiltrates, and a widened mediastinumBorio et al. JAMA 2001;286:2554-2559 [Citation ends].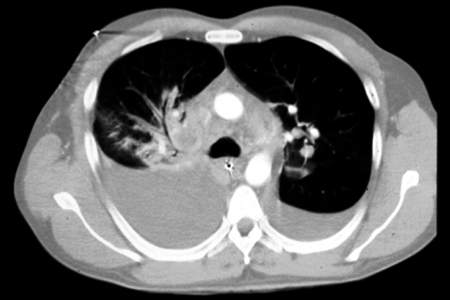
Result
enlarged, hyperdense, hilar and mediastinal lymph nodes; mediastinal edema; and large pleural effusions
Use of this content is subject to our disclaimer