Etiology
Anthrax infection is caused by the proliferation of Bacillus anthracis, a large, gram-positive, nonmotile aerobic bacillus measuring 1.0 to 1.5 micrometers by 3.0 to 10.0 micrometers.[22] Flat, white colonies grow readily on sheep's blood agar, characterized by tapered, peripheral growths known as Medusa's heads. Unlike other Bacillus species, B anthracis is nonhemolytic. In culture, organisms characteristically appear in long boxcar or cigar-shaped chains. B anthracis is also a facultative anaerobe. A prominent capsule forms in the presence of bicarbonate and carbon dioxide. Resistant 1- to 2-micrometer spores form when soil nutrients have been depleted.[23][Figure caption and citation for the preceding image starts]: Gram stain of blood in culture media. Gram-positive bacilli in chains at 20x magnification (panel A) and 100x magnification (panel B)Borio et al. JAMA 2001;286:2554-2559 [Citation ends].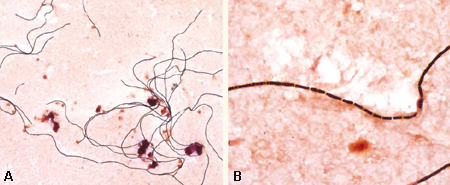
Pathophysiology
B anthracis endospores enter the body by inhalation, ingestion, injection, or most commonly, via a cut or abrasion.
The spores, initially engulfed by macrophages, germinate within these cells to become vegetative bacteria.[24] Vegetative bacteria secrete two exotoxins: edema toxin and lethal toxin. Edema toxin contains edema factor, a calmodulin-dependent adenylate cyclase responsible for inhibition of neutrophil function and the massive edema associated with cutaneous infection.[25][26][27][28] Lethal toxin is a zinc metalloprotease that stimulates the release of reactive oxygen intermediates and macrophage production of proinflammatory cytokines such as tumor necrosis factor and interleukin-1-beta; release of this toxin in systemic infection can lead to sudden death.[29][30][31] Both exotoxins are plasmid-mediated and binary, requiring a common binding protein (protective antigen) for entry into the host cell.
Cutaneous anthrax, which results from direct inoculation of spores through the skin, is a consequence of low-level, local spore germination resulting in site-specific edema and necrosis. The primary lesion develops 1-7 days after inoculation, progressing into a necrotic eschar accompanied by local edema within 48 hours.
In ingestion anthrax, which usually results from the consumption of infected meat, ingested spores also cause local disease upon germination, resulting in mucosal edema, ulceration, and ascites formation.[32] Limited oropharyngeal anthrax can also occur with ingestion of spores. In these cases, local spore deposition and germination lead to sore throat, dysphagia, cervical edema, and local lymphadenitis.
Inhalation anthrax, which results from the ingestion of aerosolized spores, is often more severe and may lead to systemic infection. Inhaled spores are engulfed by alveolar macrophages and are transported to mediastinal and peribronchial lymph nodes as they germinate. Triggers responsible for germination are unclear as spores can remain dormant for 2-43 days after exposure.[7]B anthracis bacilli subsequently multiply in regional lymph nodes, leading to pulmonary lymphedema and hemorrhagic mediastinitis. Hematogenous dissemination results in toxemia, septicemia, and death.
Injection anthrax, resulting from injection of heroin contaminated with B anthracis spores, is a more recently described form of the disease.[1]
In rare instances, lymphatic or hematogenous spread of B anthracis may also be a complication of cutaneous or ingestion anthrax. Systemic disease from any form of anthrax can result in anthrax meningitis, characterized by extensive cerebral edema, inflammatory and hemorrhagic infiltration, and rapid neurologic degeneration.[33]
Classification
Centers for Disease Control and Prevention: clinical description[2]
Cutaneous anthrax
The first symptom is usually a small, painless, pruritic papule on an exposed surface. This progresses through a vesicular stage into a depressed black eschar, which is often surrounded by edema or erythema and may be accompanied by lymphadenopathy. Fever is also common.
Inhalation anthrax
Biphasic illness. Early nonspecific symptoms include fever and fatigue. Localized thoracic symptoms (cough, chest pain, and shortness of breath) and nonthoracic symptoms (nausea, vomiting, abdominal pain, headache, diaphoresis, and altered mental status) may follow. Lung sounds are often abnormal, and imaging often shows pleural effusion or mediastinal widening.
Ingestion anthrax
Gastrointestinal: when anthrax spores germinate in the lower gastrointestinal tract, symptoms include vomiting or diarrhea (either of which may contain blood), abdominal pain, nausea, and abdominal swelling. Less specific symptoms such as fever, fatigue, and headache are also common. Altered mental status and ascites may be observed.
Oropharyngeal: when anthrax spores germinate in the oropharynx, a mucosal lesion may appear in the oral cavity or oropharynx. Symptoms include sore throat, difficulty swallowing, and swelling of the neck. Less specific symptoms include fever, fatigue, shortness of breath, abdominal pain, and nausea/vomiting; symptoms may therefore resemble a viral respiratory illness. Cervical lymphadenopathy, ascites, and altered mental status may be observed.
Injection anthrax
Usually presents after an injection as a severe soft tissue infection manifested as significant edema or bruising. No eschar is apparent, and pain is often not described. Nonspecific symptoms such as fever, shortness of breath, or nausea are sometimes the first indication of illness. Occasionally patients present with meningeal or abdominal involvement. Coagulopathy is not unusual.
Anthrax meningitis
May complicate any form of anthrax, and may also be a primary manifestation. Primary symptoms include fever, headache (often severe), nausea, vomiting, and fatigue. Usually presents with meningeal signs (e.g., meningismus), altered mental status, and other neurologic signs such as seizures or focal signs. Most patients with anthrax meningitis have cerebrospinal fluid (CSF) abnormalities consistent with bacterial meningitis, and the CSF is often described as hemorrhagic.
Signs of systemic involvement can occur with all types of anthrax.
Use of this content is subject to our disclaimer