Approach
It is clinically useful to first consider broad categories of illnesses, after clues are obtained from the history and general and neurological exams. It is helpful to think anatomically and physiologically and to develop a focused approach that will narrow the diagnostic possibilities to a few that can be sorted out with appropriate investigations.[72][73][74]
History
Just as with awake and communicative patients, the history is vital. This must be obtained from relatives, friends, and eyewitnesses, by phone if necessary. How the patient fell sick or collapsed can give important clues:
Did the patient have a seizure?
Was trauma involved?
Did the patient lose consciousness gradually or was there fluctuation, as might be seen in metabolic disorders or subdural hematoma?
Was the patient febrile or having chills (suggesting a central nervous system or systemic infection)?
The background of the patient can be important. Did the patient have cancer, profound depression (raising the possibility of drug overdose), or a history of drug or alcohol abuse? Is there an underlying illness, such as diabetes mellitus, adrenal, hepatic, or renal failure, or immunosuppression (either drug-induced or acquired)? What drugs was the patient taking? Hospital records can be helpful, as can medical alert bracelets or other medical information on his/her person.
Symptoms of herniation syndromes
It is important to recognize the features of herniation syndrome in patients with mass lesions (e.g., brain abscess, tumor, intracerebral hemorrhage, trauma with intracerebral or extracerebral hematoma).
Subfalcine herniation may produce drowsiness with progressive loss of consciousness, one-sided weakness, and/or late visual disturbances.
Uncal herniation may produce early visual disturbances before loss of consciousness.
Central (diencephalic) herniation may produce drowsiness with progressive impairment of consciousness and late visual disturbances.
Rostrocaudal herniation may produce abrupt loss of consciousness with visual disturbances, hearing disturbances, taste disturbances, difficulty swallowing, and/or differences in facial expression/movement.
Tonsillar herniation may produce difficulty breathing followed by coma.
Period of delirium
May be present in patients with various metabolic or toxic encephalopathies, including encephalopathy associated with sepsis or the systemic inflammatory response syndrome and with disorders of body temperature (hypothermia and hyperthermia).
Characterized by the inability to sustain, focus, or shift attention as its principal or essential feature. Other common phenomena include disorientation, poor short-term memory, disturbed wake-sleep cycle, agitation, confusion, and hallucinations or delusions. It is important to recognize, investigate, and treat cases of delirium promptly, before further deterioration (associated with increased mortality) occurs.
Amnesia
This is the inability to lay down new memories for a variable period (minutes to days) after the injury.
Concussion is often accompanied by an anterograde posttraumatic amnesia.
Amnesia following impairment of consciousness can also be found in some cases of transient metabolic disturbance, such as hypoglycemia, or intoxication with alcohol or sedative drugs.
Seizures, especially generalized convulsive or focal unaware seizures of temporal lobe origin, can also disrupt memory mechanisms for minutes to hours or more.
Over two-thirds of patients with aneurysmal subarachnoid hemorrhage (SAH) experience anterograde amnesia, and 17% have retrograde amnesia for time before the ictus.[75]
Psychogenic "fugue states/twilight states" are typically associated with amnesia.
Amnesia can follow vertebrobasilar ischemic attacks if the thalamus suffers a more protracted ischemic time. However, this is rare.
If the medial-inferior aspects of the both temporal lobes are infarcted following ischemic stroke, the patient will have severe memory impairment.
Duration of unconsciousness
Syncope, seizure, and concussion usually induce transient coma.
Diffuse axonal injury (DAI) causes loss of consciousness at the time of the trauma, but the duration of coma is much longer than with concussion. Patients usually regain eye opening within 2 to 3 weeks, which is related to the recovery of function of the subcortical arousal systems. The recovery of awareness is variable, ranging from mild impairment to the persistent/permanent vegetative state (unresponsive wakefulness syndrome [UWS]).
Prodromal symptoms
May be present with syncope and seizure. These are often nonspecific (e.g., nervousness or irritability, the desire to be alone).
Presence of convulsions
Convulsions may be present with numerous conditions including:
syncope (minor)
seizures/epilepsy
hypoglycemia, hyperglycemia (especially the nonketotic variety)
encephalitis
cerebral vein thrombosis (if there is cortical vein involvement), other structural brain lesions affecting the cerebral cortex or underlying white matter
hyponatremia, hypocalcemia, hypomagnesemia
profound hepatic failure
uremia
hypertensive encephalopathy (including posterior reversible encephalopathy syndrome [PRES])
the use of convulsant drugs or agents (cocaine, amphetamines, aminophylline, lidocaine, isoniazid),
advanced neurodegenerative conditions
psychogenic unresponsiveness (pseudoseizures/psychogenic seizures).
Incontinence
May occur with either syncope or seizures.
Vision disturbances
Patients with basilar artery thrombosis may present with symptoms of occipital lobe ischemia (photopsia, vision loss).
Patients with hypertensive encephalopathy may have cortical blindness and convulsive seizures if PRES develops.
Seizures may cause vision loss due to interference with incoming visual information.
Hallucinations
Elementary visual hallucinations (e.g., flashing lights in the opposite visual field) may be induced by seizures involving the occipital region.
Seizures in visual association areas often produce more complex distortions of images: for example, shapes, micropsia, or macropsia (distortions of size).
More complex visual hallucinations may occur in patients with withdrawal states of psychoses. These patients do not usually have insight into their hallucinations.
May be present in patients with recreational drug use.
Headache
Headache and nuchal rigidity may be described by noncomatose patients with meningitis or SAH.
Cerebral venous thrombosis may be considered with headache of subacute onset that is intractable and worsening and often associated with nausea and vomiting.
Headaches are less helpful in other conditions, such as trauma, hypoglycemia, systemic inflammatory diseases, large vessel ischemic strokes, seizures, and withdrawal states.
Overseas travel
Patients with encephalitis may have a history of overseas travel.
Malnutrition
Patients with Wernicke encephalopathy have a history compatible with vitamin B deficiency (usually people with alcohol dependence, nutritionally deprived patients, those with gastric stapling, or patients on hemodialysis not taking supplemental B vitamins).
Refeeding syndrome due to hypophosphatemia occurs in patients with previous malnutrition who have had in-hospital feeding.
Carbon monoxide poisoning
Common in winter months with increased use of heaters.
Also common in patients attempting suicide by shutting themselves in a garage with a car engine running.
Significant past medical history
May provide clues to the diagnosis of organ failure encephalopathies, electrolyte disorder encephalopathies, brain tumor, postinfectious encephalitis, and other causes of coma.
Drug history
May reveal ingestion/overdose of the following agents that may induce coma: ephedrine, pseudoephedrine, opioids, alpha-2 agonists, sedatives, first-generation antihistamines, tricyclic antidepressants, benztropine.
[Figure caption and citation for the preceding image starts]: The principal toxidromes, a constellation of features peculiar to certain classes of drugsTable created by G. Bryan Young, MD; used with permission [Citation ends].
History of substance abuse, poisoning
May reveal abuse/overdose of the following substances that may induce coma: lysergic acid diethylamide (LSD), cocaine, amphetamines, opioids, sedatives, organophosphates, carbamate insecticides, jimson weed, deadly nightshade, alcohol, methanol, ethylene glycol (antifreeze).
May indicate the presence of psychogenic unresponsiveness.
Focused general examination
The general exam can give important clues.
Blood pressure
Marked hypertension may indicate hypertensive encephalopathy or posterior reversible encephalopathy syndrome (PRES). Blood pressure in hypertensive encephalopathy is acutely/subacutely elevated to levels that overcome cerebral autoregulation (e.g., 240/130 mmHg).
Hypotension may indicate hypovolemic shock.
Pulse oximetry
In carbon monoxide poisoning, pulse oximetry may overestimate oxygen concentrations.
Core temperature
Coma is usually induced at core temperatures <82.4°F (28°C) and those >107.6°F (42°C).
Core temperature <82.4°F (28°C) may be present in patients with environmental hypothermia, hypothyroidism, Wernicke encephalopathy, advanced sepsis, or sedative drug intoxication.
Core temperature >104°F (40°C) may be present in patients with environmental hyperthermia, cocaine or amphetamine abuse, convulsive status epilepticus, use of anticholinergic medications, stroke, trauma, thyroid storm, or encephalitis.
Skin
Jaundice, distended veins around the umbilicus, or spider nevi suggest chronic liver failure.
Pallor, cyanosis.
Cherry red discoloration of the lips suggests carbon monoxide poisoning, but this is a rare sign and should not be relied on.
Petechial bleeding raises the possibility of a seizure, thrombotic thrombocytopenic purpura, meningococcal septicemia, Rocky Mountain spotted fever, vasculitis, or septic emboli.
Needle marks suggest drug abuse.
Head/face
May be signs of a basal skull fracture with hemotympanum, Battle sign (bruising over the mastoids), and raccoon eyes (indicating a fracture of the orbital roof).
A bitten tongue is presumptive evidence of a convulsive seizure.
A preretinal hemorrhage should raise suspicion of a ruptured intracranial aneurysm.
Roth spots in the retina may signify endocarditis, leukemia, or septic emboli.
Buccal pigmentation could indicate underlying adrenal insufficiency.
The presence of a goiter or Graves ophthalmopathy should prompt suspicion of thyroid storm.
Coma scoring scales
The Glasgow Coma Scale and Full Outline of UnResponsiveness (FOUR) scoring system are commonly used.[76][77]
Glasgow Coma Scale (GCS)
The GCS is commonly used to grade the severity of the impairment of consciousness.[76] [ Glasgow Coma Scale Opens in new window ] The FOUR scoring system evaluates additional neurological elements compared with the GCS, and appears to be equally reliable.[78] The FOUR Score Opens in new window Additionally, the FOUR scoring system is applicable in intubated patients, patients unable to respond verbally, and in those patients with abnormal respiratory pattern.[76][78] Administering the FOUR score requires an experienced assessor and may take more time than the GCS.
Focused neurological examination
It is important to localize the anatomical-physiological site of the coma. Usually if the brainstem functions are preserved the site is more rostral or the brain has been affected in a diffuse manner that relatively spares the more resistant cranial nerve nuclei. However, there are some caveats. Some specific aspects of findings on neurological exam are worth noting.
Responsiveness
Scoring systems that are more detailed than GCS are used in the ICU setting. For example, the FOUR scoring system includes eye movements, including tracking, and some motor responses (e.g., myoclonus) that are not captured by the GCS system.[77][78]
The motor response varies with the depth and severity of impairment of consciousness and the affected level of the neuraxis.
A localizing response, for example toward an irritating stimulus, especially crossing the midline, indicates a lesser degree of impairment than posturing (decorticate or decerebrate) or no response.
Visual tracking of a mirror that reflects back the image of the face or eyes of the patient differentiates a lighter degree of impaired consciousness from that of coma or vegetative state (UWS).[79]
Patients with carbon monoxide poisoning usually have intact brainstem reflexes with impaired consciousness.
Pupillary reflexes
Pupils may be unreactive in patients with hypothermia.
Can be affected with drugs that have anticholinergic properties; for example, massive overdoses of tricyclic antidepressants.
All brainstem reflexes, including pupillary responses, may be reversibly abolished with massive overdoses of barbiturates, profound hypoglycemia, or anoxic-ischemic encephalopathy. The reversibility of lost brain functions varies; these conditions can cause neuronal death if the insult is severe and prolonged.
Pupils can be small but reactive in opioid intoxication.
Pupils are initially small with central (diencephalic) herniation.
Patients with basilar artery thrombosis may have pupillary palsies.
Patients with concussion often undergo a transient impairment of brainstem function, including loss of pupillary and corneal reflexes.
The vestibular-ocular reflex (VOR)
Tested with oculocephalic (quick turn of head from side to side or in the anterior-posterior plane) or oculovestibular (ice water injection into external ear canal) procedures. These procedures stimulate and test the integrity of the semicircular canals of the inner ear, and the brainstem connections linking the vestibular nuclei, gaze centers, and III and VI cranial nerve nuclei.
May be impaired with herniation syndromes.
Can be selectively impaired in Wernicke encephalopathy, without affecting pupillary or other cranial nerve reflexes. This happens because there is a selective involvement of gray matter structures adjacent to the ventricles and cerebral aqueduct in Wernicke encephalopathy; including the vestibular nuclei involved in the VOR.
Large or cumulative doses of sedative drugs can selectively and transiently abolish the VOR.[80]
Patients with basilar artery thrombosis may have ocular palsies.
Not tested in trauma patients until cervical spine injuries have been ruled out.
Profound neuromuscular weakness
Hypophosphatemia, when acute and profound, can be similar to Guillain-Barre syndrome. This can be seen in the refeeding syndrome, in which there is an increased shift of phosphate into cells after a glucose load in severely malnourished patients.[81]
Flaccid quadriplegia is also sometimes a feature of acute, severe hypokalemia or hypomagnesemia.
Patients with basilar artery thrombosis may have pseudobulbar palsy and/or quadriparesis.
Patients with subfalcine herniation + diencephalic displacement may have associated signs of hemiparesis.
Those with West Nile encephalitis may have bulbar paralysis and quadriplegia due to the involvement of motor neurons.
In locked-in states, consciousness is preserved but motor output is impaired:
Basis pontis lesions: upper motor neuron palsy of lower cranial nerves (pseudobulbar palsy) and 4 limbs, vertical eye movement, eyes open and close voluntarily
Polyneuropathy: no vertical eye movement, may lose pupillary reflexes, absent deep tendon reflexes
Pharmacologic paralysis: intact pupillary reflexes.
Seizures
Most commonly myoclonic (with bilaterally synchronous jerks, distinct from multifocal myoclonus), can occur in a number of metabolic encephalopathies, including hyponatremia, hyperosmolar states (especially in nonketotic hyperglycemia, where seizures can be misleadingly focal), hypocalcemia, extreme hypercalcemia, uremia, advanced hepatic encephalopathy, and hypoglycemia, and in postresuscitation encephalopathy after cardiac arrest. In the latter situation, myoclonic status epilepticus is often fatal, without recovery of awareness.[82] This is due to widespread neuronal death in a pattern that is very distinct from the pattern of neuronal loss after status epilepticus.[83]
Signs of herniation syndromes
Subfalcine herniation may produce progressive impairment of consciousness with/without hemiparesis, and late oculomotor palsy.
Uncal herniation may produce early oculomotor palsy before impaired consciousness.
Central (diencephalic) herniation may produce initially small pupils and then impairment of consciousness, with late irreversible oculomotor palsy.
Rostrocaudal herniation may produce abrupt loss of consciousness with cranial nerve palsies.
Tonsillar herniation may produce respiratory arrest followed by hypertension, then hypotension, coma and often brain death.
Oculomotor signs associated with herniation include:
Gaze preference or conjugate eye deviation to one side initially.
Followed by pupillary asymmetry due to stretching of the third (oculomotor) cranial nerve over the clivus on the side of the mass.
This usually manifests as dilation of the pupil ipsilateral to the lesion (note that about 20% of people have anisocoria). This is followed by loss of ipsilateral pupillary reactivity and paralysis of adduction of the eye.
In later stages the opposite pupil loses its reactivity, due to intrinsic midbrain damage from herniation.
Laboratory investigations
Arterial or capillary blood gas determination can be very helpful in the presence of hyperventilation and occasionally in hypoventilation and for some toxidromes. ABG analysis is readily available and of some confirmatory value in psychogenic unresponsiveness. In pseudoseizures, blood gases are usually normal or may show a respiratory alkalosis from hyperventilation, as opposed to the profound, mixed metabolic-respiratory acidosis of a convulsive seizure. The correlation of basic respiratory patterns with blood gas determination can narrow the differential diagnostic possibilities considerably.
Hyperventilation with metabolic acidosis: possible causes include uremia, diabetic ketoacidosis, lactic acidosis, or poisoning with salicylates, methanol, or ethylene glycol.
Hyperventilation with respiratory alkalosis: possible causes include liver failure, acute sepsis, any cardiopulmonary state that causes hypoxemia, the acute phase of salicylate poisoning, or psychogenic hyperventilation.
Hypoventilation with respiratory acidosis: coma occurs only if there is severe hypercapnia. Causes include respiratory failure due to either central or peripheral nerve disease, and chest conditions or deformities.
Hypoventilation with metabolic alkalosis: consciousness is usually not impaired. Causes include vomiting and alkali ingestion, but psychogenic unresponsiveness or an additional cause should be suspected if the patient is unconscious.
[Figure caption and citation for the preceding image starts]: Respiratory abnormalities, blood gas determination, and diagnostic possibilitiesTable created by G. Bryan Young, MD; used with permission [Citation ends].
Serum glucose, calcium, sodium, potassium, magnesium, phosphate, urea, and creatinine should be checked to evaluate the cause of syncope, fainting, or seizure and to assess for the presence of electrolyte disorders.
Once the differential has been narrowed, further laboratory tests can be performed according to the suspected cause.
Liver function tests should be done if hepatic failure is suspected.
International normalized ratio (INR) is sensitive to acute hepatocellular failure.
"Drug screen" is rarely comprehensive but can be specified to include alcohol, benzodiazepines, barbiturates, opioids, cocaine, amphetamines, tricyclic antidepressants, salicylates, acetaminophen, and other agents. Some drugs, such as antihistamines, may not have an available assay and one must go on clinical suspicions.
Blood cultures should be done in the presence of fever or hypothermia.
Blood carboxyhemoglobin level is required if carbon monoxide poisoning is suspected, bearing in mind that smokers may have slightly elevated levels.
Pyruvate and serum thiamine should be measured if Wernicke encephalopathy is suspected.
Specific drug or metabolic assays can be done in special circumstances.
Imaging
Imaging is essential when there is a strong possibility of a structural brain lesion or for diagnosing specific disorders. A CT head scan is most commonly used, as it is quick, available, and requires less preparation than an MRI scan; however, MRI can provide more detail. Consensus recommendations from the American College of Radiology support noncontrast CT for adult patients with new unexplained altered mental status and suspected intracranial pathology or focal neurologic deficit.[84]
CT is sensitive to intracranial hemorrhages, major shifts of midline structures, and mass effect. Patients with mass lesions (e.g., brain abscess, tumor, intracerebral hemorrhage, trauma with intracerebral or extracerebral hematoma) and herniation syndrome require urgent imaging. An unenhanced CT is usually performed first, then contrast CT if necessary to clarify the nature of mass (e.g., differentiating tumor from brain abscess).
MRI is usually performed later and can be helpful in showing multiple lesions (e.g., metastases) and their nature (e.g., infarctions vs inflammatory or neoplastic lesions).
Focal signs, such as a hemiparesis or an oculomotor palsy in a comatose patient, should also prompt a scan. However, coma may precede such focal signs in patients with supratentorial mass lesions. Thus, neuroimaging is also indicated when structural lesions are possible or if the diagnosis is uncertain.
Imaging in patients with traumatic brain injury and suspected intracranial injury
Consensus recommendations from the American College of Radiology support noncontrast CT use as a first-line imaging modality in patients with traumatic brain injury.[85]
Key recommendations from the National Institute for Health and Care Excellence (NICE) guideline for head injury management:[17]
Refer to neurosurgical center if any of the following are present:
Persisting coma: GCS score 8/15 or less after initial resuscitation
Unexplained confusion that persists for more than 4 hours
Deterioration in level of consciousness after admission
Progressive focal neurologic signs
A seizure without full recovery
Definite or suspected penetrating injury
Cerebrospinal fluid (CSF) leak.
For people aged 16 years and over, a CT head scan is needed within 1 hour if any of the following is present:[17]
GCS of 12 or less on initial assessment in the emergency department
GCS less than 15 at 2 hours after the injury
Suspected open or depressed skull fracture
Any sign of basal skull fracture (hemotympanum, ‘panda’ eyes, cerebrospinal fluid leakage from the ear or nose, Battle sign)
Post-traumatic seizure
Focal neurological deficit
More than one episode of vomiting
For people aged 16 years and over who have had some loss of consciousness or amnesia since the injury, CT head should be performed within 8 hours (or within the hour in someone presenting more than 8 hours after the injury) if any of the following are present:[17]
Age 65 years or older
Any history of bleeding or clotting disorders
Dangerous mechanism of injury (e.g., a pedestrian or cyclist struck by a motor vehicle, an occupant ejected from a motor vehicle, or fall from a height greater than 1 meter or 5 stairs)
More than 30 minutes retrograde amnesia of events immediately before the head injury
For people under 16 years who have sustained a head injury, CT head should be performed within 1 hour of any of the following risk factors being identified:[17]
Suspicion of nonaccidental injury
Posttraumatic seizure
On initial emergency department assessment, a GCS score <14 or, for infants under 1 year, a GCS score (pediatric) <15
At 2 hours after the injury, a GCS score <15
Suspected open or depressed skull fracture, or tense fontanel
Any sign of basal skull fracture (hemotympanum, “panda” eyes, cerebrospinal fluid leakage from the ear or nose, Battle's sign)
Focal neurologic deficit
For infants under 1 year, a bruise, swelling, or laceration of more than 5 cm on the head.
For people under 16 years who have sustained a head injury and have more than one of these risk factors, CT head should be performed within 1 hour of the risk factors being identified:[17]
Loss of consciousness lasting more than 5 minutes (witnessed)
Abnormal drowsiness
3 or more discrete episodes of vomiting
Dangerous mechanism of injury (high-speed road traffic accident as a pedestrian, cyclist or vehicle occupant, fall from a height of more than 3 metres, high-speed injury from a projectile or other object)
Amnesia (anterograde or retrograde) lasting more than 5 minutes (it is not possible to assess amnesia in children who are preverbal and is unlikely to be possible in children under 5)
Any current bleeding or clotting disorder.
People under 16 years who have sustained a head injury but have only one of the above risk factors (beginning Loss of consciousness lasting more than 5 minutes [witnessed]) should be observed for a minimum of 4 hours in a hospital. If, during observation, any of the following risk factors are identified, CT head should be performed within 1 hour:[17]
A GCS score <15
Further vomiting
A further episode of abnormal drowsiness.
If none of these risk factors occur during observation, clinical judgement should be used to determine whether a longer period of observation is needed.[17]
Imaging in anticoagulated patients
Several guidelines recommend, or suggest consideration of, CT head imaging for anticoagulated patients after minor head injury, regardless of symptoms.[17][86][87]
NICE recommends consideration of a CT head scan for those with a head injury who are taking an anticoagulant or antiplatelet medication (and have no other indication for a CT head scan):[17]
within 8 hours of the injury
within the hour if they present more than 8 hours after the injury.
[Figure caption and citation for the preceding image starts]: Brainstem hemorrhage in the midbrain that extended from a hypertensive hemorrhage in the ponsFrom the personal collection of G. Bryan Young, MD; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Hypertensive hemorrhage in the pons that ruptured into the fourth ventricle and extended into the midbrainFrom the personal collection of G. Bryan Young, MD; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Hypertensive hemorrhage in the pons that ruptured into the fourth ventricle and extended into the midbrainFrom the personal collection of G. Bryan Young, MD; used with permission [Citation ends].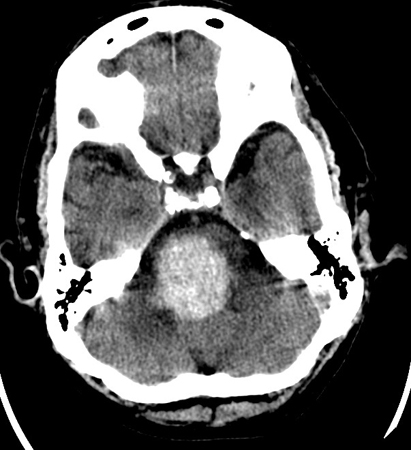
Lumbar puncture and CSF analysis
Lumbar puncture is indicated if there is suspicion of meningitis, especially bacterial, fungal, or tuberculous, and for detecting meningeal cancer. Lumbar puncture can also confirm SAH from a ruptured aneurysm when CT has not detected it (5% of cases). Xanthochromia, a yellow staining of the CSF from hemoglobin breakdown products, can be suspected clinically and confirmed by spectrophotometry.
More specific diagnostic testing, apart from culture, stains, cytology, and flow cytometry, includes:
polymerase chain reaction (PCR) for herpes simplex virus (HSV) 1 and 2
broad-range bacterial PCR
specific meningeal pathogen PCR
PCR for Mycobacterium tuberculosis
reverse transcriptase (RT) PCR for enteroviruses
PCR for West Nile virus
PCR for Epstein-Barr virus
PCR for varicella zoster virus
PCR for cytomegalovirus DNA
PCR for HIV RNA
RT-PCR for rabies virus.
Antigen screening can be done for cryptococcal and histoplasma polysaccharide antigens. Antibody screens in the CSF are available for HSV (serum-to-CSF antibody ratio of <20:1), arthropod-borne viruses, Borrelia burgdorferi (for suspected Lyme disease), and rabies virus; complement fixation antibody testing for Coccidioides immitis can also be performed. CSF analysis may also help in the diagnosis of acute inflammatory demyelinative polyneuropathy (in cases of locked-in state).
EEG
EEG can be of great help in detecting seizures; it seems appropriate to request one, even in the ER, when the cause of coma is not apparent and brainstem reflexes are intact. Evidence suggests that at least 14% of patients who did not wake after a convulsive seizure were in nonconvulsive status epilepticus (NCSE).[88]
Seizures may also be acquired in the ICU, especially in those with structural brain lesions. It has been demonstrated that at least 8% of patients comatose from brain injury are in NCSE.[35][89] Most often this is undetectable without EEG. Because status epilepticus can damage the brain, it is important that seizures be detected early and treated promptly and effectively. The liberal use of EEG in the ICU is helpful; continuous monitoring for at least 72 hours increases NCSE diagnostic yield and, in patients with seizures, provides feedback that the seizures are controlled and that the sedation/anesthesia is not excessive.
EEG is also helpful for diagnosing pseudoseizures or psychogenic seizures (in patients with psychogenic unresponsiveness), acute herpes simplex encephalitis (sensitive in >80% of cases), hypothermia, hyperthermia, SAH, and inflammatory processes (e.g., burns).[24]
EEG demonstrates different patterns (e.g., slow pattern, burst-suppression pattern, isoelectric pattern). These features are not specific to etiology and are mainly used to grade the severity of the encephalopathy. The most profound abnormality is generalized suppression of voltage/electrocerebral silence, then a burst-suppression pattern. These are common in very severe cases of anoxic-ischemic encephalopathy after cardiac arrest, but they may be found in more reversible encephalopathies due to overdose of barbiturates, benzodiazepines, anesthetic agents, or profound hypothermia. Diffuse slowing with rhythmic waves or triphasic waves indicates a somewhat less severe but still profound encephalopathy, usually but not invariably due to metabolic derangements: for example, uremia, hepatic failure, or sepsis.
Electromyography (EMG)
In cases of unresponsiveness, EMG can help exclude a neuromuscular cause. For example, neuromuscular blockade from the prolonged action of muscle relaxants and profound, diffuse polyneuropathies (e.g., acute inflammatory demyelinative polyneuropathy and the axonal form of Guillain-Barre syndrome).
Prognostic tests
The prognosis of patients with severe diffuse axonal injury (DAI) can be estimated using:
Somatosensory evoked response testing, which uses a single sensory pathway and has been shown to be sensitive and specific
Magnetic transcranial cortical motor stimulation, which can be used to assess the corticospinal motor integrity, although this use has not yet been standardized[90]
Diffusion tensor imaging, which offers promising prognostic strategy, especially when used in combination with somatosensory evoked responses[91]
Metabolic studies, which demonstrate glucose uptake and metabolism in gray and white matter of the brain using positron emission tomography (PET) scanning, may be clinically useful, but this is yet to be determined.[92][93]
The prognosis of patients with anoxic-ischemic encephalopathy after cardiac arrest can be estimated using:
Somatosensory evoked response testing, which shows bilateral absence of the N20 response (from the primary sensory cortex) to median nerve stimulation of the wrist[94]
Serum neuronal specific enolase >33 micrograms/L between days 1 and 3 reliably predicts an outcome no better than severe disability requiring long-term nursing home care.[95]
The prognosis of patients with carbon monoxide poisoning may be estimated using:
Single-photon emission CT during the later stages.
The prognosis of patients in coma is often difficult. However, some advances have been made in the application of ancillary testing:
Somatosensory evoked potential holds promise in both children and adults[96][97]
Diffusion tensor imaging (DTI) allows for the evaluation of fiber tracts, taking advantage of the anisotropic motion of water within the axons (fractional anisotropy). Studies of mild traumatic brain injuries have shown abnormalities in the genu of the corpus callosum. DTI is beginning to be used clinically in traumatic brain injuries.[98]
Use of this content is subject to our disclaimer