Tests
1st tests to order
CT abdomen/pelvis
Test
Radiologic assessment of potential lesions using CT (with or without contrast) is the definitive test for initial diagnosis and staging of RCC.[1][64] Contrast-enhanced CT with renal protocol has been found to have 100% specificity and ≥90% sensitivity for characterizing a renal mass as malignant.[68] There is evidence to suggest the overall accuracy of tumor extent on CT is 93% specific and 96% sensitive when compared with final pathologic staging; accuracy is 99% specific for adrenal involvement but with variable positive predictive values (35% to 92%); there is a 10% false-negative rate and a 58% false-positive rate for lymph node assessment.[68][Figure caption and citation for the preceding image starts]: CT scan showing localized right upper pole kidney cancerFrom the collection of M. Jewett; used with permission [Citation ends].
Result
renal mass, regional lymphadenopathy, and/or visceral/bone metastases
CT chest
MRI abdomen/pelvis
Test
MRI (with and without contrast) is the modality of choice for diagnosis and staging in patients where contrast dye is contraindicated (due to renal insufficiency or allergy).[64] Can be used as an adjunct to CT to better assess adrenal invasion and vena cava involvement by tumor or thrombus (found to be 94% accurate for thrombus).[68] MRI may be more useful than CT in assessing potential benign lesions such as angiomyolipoma.[69]
Result
renal mass, regional lymphadenopathy, and/or visceral/bone metastases
abdominal/pelvic ultrasound
Test
Diagnosis is usually suggested by ultrasound.[2] However, it is not possible to assess complex cystic masses and/or solid renal masses with ultrasound alone.
Overall detection rate for RCC is as low as 71% with conventional ultrasound, whereas contrast-enhanced ultrasound may be much more accurate (100% diagnostic rate in one study).[70]
Ultrasound can be used to detect cystic and solid renal lesions, and determine if cystic renal lesions are benign, but it is less accurate than MRI and CT, especially in detecting smaller lesions and characterizing more complex renal masses especially in hereditary syndromes prone to cystic disease (e.g., VHL).[62][63]
If lesions are detected on abdominal ultrasound performed for other indications, the next investigation should be CT or MRI of the abdomen and pelvis.[61]
Result
abnormal renal cyst/mass, lymphadenopathy, and/or other visceral metastatic lesions
CBC
Test
Laboratory findings in paraneoplastic syndromes may include anemia from chronic disease, and erythrocytosis from excess erythropoietin production.[18]
Result
paraneoplastic syndrome: reduced Hb, or elevated red blood cells
LDH
Test
Poor prognostic marker in advanced RCC as per the Memorial Sloan Kettering Cancer Center (MSKCC) score for metastatic RCC.[60]
Result
advanced RCC: >1.5 times the upper limit of normal
corrected calcium
Test
Poor prognostic marker in advanced RCC as per the Memorial Sloan Kettering Cancer Center (MSKCC) score for metastatic RCC.[60]
Result
advanced RCC: >10 mg/dL
liver function tests
Test
Transaminitis (elevated liver transaminases, aspartate aminotransferase/alanine aminotransferase) and/or poor liver function may be indicative of metastatic lesions.
In the absence of liver metastases, cholestasis (elevated bilirubin, alk phos, gamma-GT), with concomitant elevated prothrombin time, thrombocytosis, and hepatosplenomegaly, is a paraneoplastic presentation of RCC known as Stauffer syndrome.[18]
Result
metastatic disease/paraneoplastic syndrome: abnormal
coagulation profile
Test
In the absence of liver metastases, cholestasis (elevated bilirubin, alk phos, gamma-GT), with concomitant elevated prothrombin time (PT), thrombocytosis, and hepatosplenomegaly, is a paraneoplastic presentation of RCC known as Stauffer syndrome.[18]
Result
paraneoplastic syndrome: elevated PT
creatinine
Test
May be indicative of chronic kidney disease either preceding or due to RCC. Important to know baseline function in choosing surgical approach and/or systemic treatment.
Result
may be elevated
estimated GFR
Test
Used to determine renal function. If reduced, chronic kidney disease staging is important to guide management options and for prognosis.[1]
Result
may be reduced
urinalysis
Test
The presence or absence of nonvisible hematuria on urinalysis is not specific or sensitive for RCC diagnosis.[71] However, if found, a workup should be initiated for urinary tract pathology.[1]
Do not routinely perform cystoscopy or imaging in asymptomatic, never-smoking women younger than 50 years with microscopic hematuria who have fewer than 25 red blood cells per high-power field. This is because asymptomatic hematuria in women is less likely to be associated with malignancy compared with men.[59]
Proteinuria is neither sensitive nor specific, but the presence of significant proteinuria can indicate renal dysfunction from a variety of causes, including RCC. Proteinuria is also often seen in chronic kidney disease and hypertension, which are risk factors for RCC.
The tyrosine kinase inhibitors used for treatment of metastatic RCC can cause or exacerbate proteinuria, and thus it should be screened at least prior to starting treatment.
Result
hematuria and/or proteinuria
Tests to consider
MRI brain/spine
bone scan
Test
Only recommended if patient presents with localizing bone pain and/or elevated alk phos.[17]
Result
normal, or abnormal uptake in bone site consistent with metastases
biopsy
Test
Renal mass biopsy is not required in cases where imaging demonstrates a malignant renal mass with no evidence of distant metastatic disease, as management usually includes surgical resection and diagnosis is confirmed on surgical pathology.[1][65]
Indeterminate (and usually smaller) renal lesions found on imaging can be biopsied to support which candidates are suitable for active surveillance based on tumor histology.[72]
In advanced disease, the most easily and safely biopsied metastatic lesion can provide the diagnosis, although the renal primary is sometimes still biopsied.
Renal mass biopsy should also be considered when an alternative diagnosis (e.g., abscess) is suspected.[1][65]
Result
malignancy of various histology
surgical pathology
Test
Most common histology is clear cell RCC.[1][2] Localized renal mass is best assessed surgically (complete or partial nephrectomy), which also serves as potential definitive treatment. [Figure caption and citation for the preceding image starts]: Gross pathology showing localized right upper pole kidney cancerFrom the collection of M. Jewett; used with permission [Citation ends].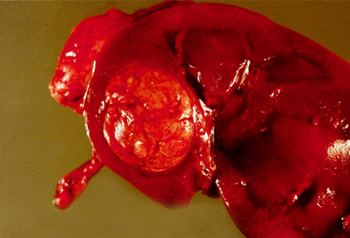
Result
malignancy of various histology
genetic evaluation
Test
Genetic testing and counseling is recommended in patients meeting the following criteria: age ≤46 years; and/or bilateral or multifocal tumors; and/or first- or second-degree relative with RCC; and/or close blood relative with a known pathogenic variant; and/or specific histologic characteristics which suggest a hereditary form of RCC (e.g., multifocal papillary histology; hereditary leiomyomatosis-associated RCC, RCC with fumarate hydratase deficiency, or other associated histologic features; multiple chromophobe, oncocytoma or oncocytic hybrid; angiomyolipomas of the kidney and one additional tuberous sclerosis complex criterion; succinate dehydrogenase-deficient RCC histology).[1][5][17][64]
Result
may suggest presence of hereditary form of RCC
Use of this content is subject to our disclaimer