RCC is often asymptomatic and therefore more commonly diagnosed after an incidental finding. More than 50% of RCCs are diagnosed incidentally; up to 40% of renal masses detected incidentally are small and localized.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
When localized malignant-appearing renal masses are detected on imaging, patients should be referred to urologists. The urologic assessment may be for active surveillance or biopsy, but most commonly for nephrectomy, which can be both therapeutic and diagnostic. Advanced disease can be referred for image-guided renal or metastatic lesion biopsy. These patients will need a referral to both a medical oncologist and a urologist (the latter for consideration of nephrectomy). Patients with known heritable syndromes may be approached with more vigilance in terms of screening, diagnosis, and follow-up.
Historical factors
Renal masses are usually only symptomatic late in the disease. The classic triad of hematuria, flank pain, and abdominal mass is uncommon (less than 10%) and is indicative of aggressive histology locally and advanced disease.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
Rarely, patients present with symptoms of metastatic disease such as bone pain or respiratory symptoms.[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
Around 10% to 40% of RCCs will develop paraneoplastic syndromes, none of which are specific to RCC.[18]Sacco E, Pinto F, Sasso F, et al. Paraneoplastic syndromes in patients with urological malignancies. Urol Int. 2009;83(1):1-11.
https://www.karger.com/Article/Pdf/224860
http://www.ncbi.nlm.nih.gov/pubmed/19641351?tool=bestpractice.com
Sequelae of these syndromes vary depending on the organ system involved, but include symptoms associated with hypercalcemia, liver dysfunction (from metastatic disease or Stauffer syndrome [liver failure due to paraneoplastic syndrome in the absence of liver metastases]), excess adrenocorticotropic hormone (ACTH), anemia, polycythemia (mediated by inappropriate erythropoietin production), and neurologic dysfunction (such as myopathy).[18]Sacco E, Pinto F, Sasso F, et al. Paraneoplastic syndromes in patients with urological malignancies. Urol Int. 2009;83(1):1-11.
https://www.karger.com/Article/Pdf/224860
http://www.ncbi.nlm.nih.gov/pubmed/19641351?tool=bestpractice.com
Patients with causative hereditary syndromes may present with dermatologic, ophthalmic, or other symptoms associated with characteristic pathology in other organ sites.
Family history may be positive for renal cancer or hereditary syndromes (e.g., von Hippel-Lidau [VHL], Birt-Hogg-Dube [BHD], type 1 papillary RCC, hereditary leiomyomatous renal cell cancer syndrome).[33]Maher ER. Hereditary renal cell carcinoma syndromes: diagnosis, surveillance and management. World J Urol. 2018 Dec;36(12):1891-8.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6280834
http://www.ncbi.nlm.nih.gov/pubmed/29680948?tool=bestpractice.com
Social history may reveal associated smoking risks and possible occupational risks (exposure to asbestos/cadmium).[30]Kabaria R, Klaassen Z, Terris MK. Renal cell carcinoma: links and risks. Int J Nephrol Renovasc Dis. 2016 Mar 7;9:45-52.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4790506
http://www.ncbi.nlm.nih.gov/pubmed/27022296?tool=bestpractice.com
Past medical history may reveal history of obesity, hypertension, or dialysis/acquired renal cystic disease.[30]Kabaria R, Klaassen Z, Terris MK. Renal cell carcinoma: links and risks. Int J Nephrol Renovasc Dis. 2016 Mar 7;9:45-52.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4790506
http://www.ncbi.nlm.nih.gov/pubmed/27022296?tool=bestpractice.com
Do not routinely perform cystoscopy or imaging in asymptomatic, never-smoking women younger than 50 years with microscopic hematuria who have fewer than 25 red blood cells per high-power field. This is because asymptomatic hematuria in women is less likely to be associated with malignancy compared with men.[59]American Urogynecologic Society. Ten things physicians and patients should question. Choosing Wisely, an initiative of the ABIM Foundation. 2021 [internet publication].
https://web.archive.org/web/20230131162755/https://www.choosingwisely.org/societies/american-urogynecologic-society
Physical exam
Physical exam has a limited role in diagnosis but may prompt further workup, and, in combination with certain laboratory findings, may be suggestive of RCC. A full physical exam may reveal evidence of local or distant disease sequelae.
Physical findings that may suggest renal malignancy are palpable abdominal masses (especially in thin people), cervical lymphadenopathy, lower leg edema suggesting venous compromise, and scrotal varicocele in men.[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
Hypertension, fever, cachexia, and paraneoplastic syndrome findings may be present, although they are not specific for RCC. Physical signs of paraneoplastic syndromes include pallor, cachexia, and myoneuropathy (muscle weakness associated with both primary muscle fiber pathology and associated nerve pathology). Signs of hepatic dysfunction may be present due to liver metastases, or Stauffer syndrome (liver failure due to paraneoplastic syndrome in the absence of liver metastases).[18]Sacco E, Pinto F, Sasso F, et al. Paraneoplastic syndromes in patients with urological malignancies. Urol Int. 2009;83(1):1-11.
https://www.karger.com/Article/Pdf/224860
http://www.ncbi.nlm.nih.gov/pubmed/19641351?tool=bestpractice.com
Physical signs of causative hereditary syndromes include papules (BHD), skin fibromas (hereditary leiomyomatous), and retinal angiomatosis (VHL).
There are currently no guidelines to recommend targeted physical exam maneuvers to screen for RCC, as none of the findings above are sensitive or specific, even in high-risk individuals.
Physical exam should include an assessment of performance status (measures patient mobility, ambulation, ability to perform self-care), which has implications for prognosis.
Laboratory investigations
Laboratory tests are required for the assessment of renal function (serum creatinine, estimated glomerular filtration rate, and urinalysis) and for completeness of metastatic evaluation.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
Lactate dehydrogenase, complete blood count, and calcium are important investigations in the workup of RCC (particularly at advanced stage), in order to assess prognosis and detect the presence of paraneoplastic syndromes.[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
[60]Motzer RJ, Bacik J, Mazumdar M. Prognostic factors for survival of patients with stage IV renal cell carcinoma: Memorial Sloan-Kettering Cancer Center experience. Clin Cancer Res. 2004 Sep 15;10(18 Pt 2):6302S-3S.
http://clincancerres.aacrjournals.org/content/10/18/6302S.long
http://www.ncbi.nlm.nih.gov/pubmed/15448021?tool=bestpractice.com
Iron and nutritional studies should be completed if anemia is found, to rule out reversible factors; the profile is often that of anemia of chronic disease.
Full biochemistry, including renal/liver function, coagulation profile, and urinalysis, is also important in screening for local or paraneoplastic complications of RCC, and for baseline organ function in anticipation of treatment.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
[60]Motzer RJ, Bacik J, Mazumdar M. Prognostic factors for survival of patients with stage IV renal cell carcinoma: Memorial Sloan-Kettering Cancer Center experience. Clin Cancer Res. 2004 Sep 15;10(18 Pt 2):6302S-3S.
http://clincancerres.aacrjournals.org/content/10/18/6302S.long
http://www.ncbi.nlm.nih.gov/pubmed/15448021?tool=bestpractice.com
If specific paraneoplastic syndromes are suspected, targeted investigations should follow. Laboratory findings in paraneoplastic syndromes may include anemia from chronic disease; erythrocytosis from excess erythropoietin; hypercalcemia from parathyroid hormone-related protein/lytic bone lesions/prostaglandin production; excess ACTH from hypercortisolism; and abnormal liver function tests from hepatic dysfunction.[18]Sacco E, Pinto F, Sasso F, et al. Paraneoplastic syndromes in patients with urological malignancies. Urol Int. 2009;83(1):1-11.
https://www.karger.com/Article/Pdf/224860
http://www.ncbi.nlm.nih.gov/pubmed/19641351?tool=bestpractice.com
Imaging
Imaging is paramount to diagnosis, regardless of presentation.
Diagnosis is usually suggested by ultrasound.[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
However, it is not possible to assess complex cystic masses and/or solid renal masses with ultrasound alone. If lesions are detected on abdominal ultrasound performed for other indications, the next investigation should be computed tomography (CT) or magnetic resonance imaging (MRI) of the abdomen and pelvis with chest imaging (CT) for staging.[61]Leveridge MJ, Bostrom PJ, Koulouris G, et al. Imaging renal cell carcinoma with ultrasonography, CT and MRI. Nat Rev Urol. 2010 Jun;7(6):311-25.
http://www.ncbi.nlm.nih.gov/pubmed/20479778?tool=bestpractice.com
Ultrasound can be used to detect cystic and solid renal lesions, and determine if cystic renal lesions are benign, but it is less accurate than MRI and CT, especially in detecting smaller lesions and characterizing more complex renal masses.[62]Meister M, Choyke P, Anderson C, et al. Radiological evaluation, management, and surveillance of renal masses in von Hippel-Lindau disease. Clin Radiol. 2009 Jun;64(6):589-600.
http://www.ncbi.nlm.nih.gov/pubmed/19414081?tool=bestpractice.com
[63]Usher-Smith J, Simmons RK, Rossi SH, et al. Current evidence on screening for renal cancer. Nat Rev Urol. 2020 Nov;17(11):637-42.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7610655
http://www.ncbi.nlm.nih.gov/pubmed/32860009?tool=bestpractice.com
Ultrasound may also be positive for uterine fibroma in patients with hereditary leiomyomatous renal cell syndrome.
Radiologic assessment of potential lesions using CT (with and without contrast) is the definitive test for initial diagnosis of renal malignancy.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[64]National Cancer Comprehensive Network. NCCN clinical practice guidelines in oncology: kidney cancer [internet publication].
https://www.nccn.org/professionals/physician_gls/default.aspx
CT is the modality of choice; MRI is an alternative, particularly if contrast is contraindicated (allergy or renal dysfunction).[64]National Cancer Comprehensive Network. NCCN clinical practice guidelines in oncology: kidney cancer [internet publication].
https://www.nccn.org/professionals/physician_gls/default.aspx
MRI is also done for better assessment of tumor encroachment into the inferior vena cava.[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: CT scan showing localized right upper pole kidney cancerFrom the collection of M. Jewett; used with permission [Citation ends].
Renal cancer most often appears as solid or complex cystic masses. CT/MRI allows for:[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
Relatively precise characterization of renal lesions
Interpretation as benign or malignant
Assessment of renal mass invasiveness, lymph node involvement, and intra-abdominal metastatic foci.
When renal lesions are detected incidentally on abdominal CT/MRI performed for other indications, findings may be sufficient to make the initial diagnosis. The Bosniak classification was designed to classify cystic renal masses into five categories based on CT/MRI radiology.[13]Israel GM, Hindman N, Bosniak MA. Evaluation of cystic renal masses: comparison of CT and MR imaging by using the Bosniak classification system. Radiology. 2004 May;231(2):365-71.
http://www.ncbi.nlm.nih.gov/pubmed/15128983?tool=bestpractice.com
All patients require chest imaging as part of staging and initial workup to evaluate for pulmonary metastases. CT is preferred; chest x-ray is indicated if CT is unavilable.[64]National Cancer Comprehensive Network. NCCN clinical practice guidelines in oncology: kidney cancer [internet publication].
https://www.nccn.org/professionals/physician_gls/default.aspx
Further metastatic workup is only performed if metastasis is indicated by clinical or laboratory findings.[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
[64]National Cancer Comprehensive Network. NCCN clinical practice guidelines in oncology: kidney cancer [internet publication].
https://www.nccn.org/professionals/physician_gls/default.aspx
For example, a bone scan can be done for bone pain or elevated alkaline phosphatase. MRI brain may be indicated for localizing neurologic signs and symptoms, or when systemic therapy or cytoreductive nephrectomy is being considered in patients with metastases.[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
[Figure caption and citation for the preceding image starts]: Bosniak classificationTable created by Rodrigo R. Pessoa MD; used with permission [Citation ends].
Histopathology (surgical resection or biopsy)
If CT/MRI demonstrates a malignant renal mass with no evidence of distant metastatic disease, biopsy is not routinely indicated (as it is unlikely to alter management and patients are usually counseled to proceed with surgical resection and diagnosis is confirmed on surgical pathology).[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[65]Lavallée LT, McAlpine K, Kapoor A, et al. Kidney Cancer Research Network of Canada (KCRNC) consensus statement on the role of renal mass biopsy in the management of kidney cancer. Can Urol Assoc J. 2019 Dec;13(12):377-83.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6892686
http://www.ncbi.nlm.nih.gov/pubmed/31799919?tool=bestpractice.com
The role of biopsy for indeterminate localized renal masses is, however, controversial. Evidence suggests there may be a role for surveillance of small renal masses (SRMs) <4 cm in individuals with certain tumor histologies on biopsy at diagnosis; however, biopsy is less accurate in smaller lesions.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[65]Lavallée LT, McAlpine K, Kapoor A, et al. Kidney Cancer Research Network of Canada (KCRNC) consensus statement on the role of renal mass biopsy in the management of kidney cancer. Can Urol Assoc J. 2019 Dec;13(12):377-83.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6892686
http://www.ncbi.nlm.nih.gov/pubmed/31799919?tool=bestpractice.com
Typically, if metastatic disease is found on staging, biopsy of the most accessible metastatic lesion is performed to make the diagnosis. However, if nephrectomy is still being considered, surgical pathology is sufficient. Finally, biopsy of a renal mass may also be required to confirm renal metastases from another primary malignancy for staging purposes or if another diagnosis (e.g., abscess), is suspected.[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[65]Lavallée LT, McAlpine K, Kapoor A, et al. Kidney Cancer Research Network of Canada (KCRNC) consensus statement on the role of renal mass biopsy in the management of kidney cancer. Can Urol Assoc J. 2019 Dec;13(12):377-83.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6892686
http://www.ncbi.nlm.nih.gov/pubmed/31799919?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Gross pathology showing localized right upper pole kidney cancerFrom the collection of M. Jewett; used with permission [Citation ends].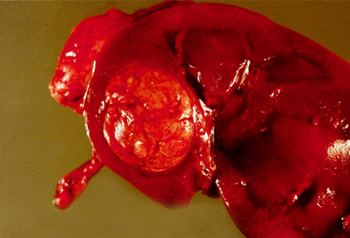
Genetic evaluation
Genetic testing and counseling is recommended in patients meeting the following criteria:[1]American Urological Association. Renal mass and localized renal cancer: evaluation, management, and follow up. 2021 [internet publication].
https://www.auanet.org/guidelines/guidelines/renal-mass-and-localized-renal-cancer-evaluation-management-and-follow-up
[5]Richard PO, Violette PD, Bhindi B, et al. Canadian Urological Association guideline: management of small renal masses - full-text. Can Urol Assoc J. 2022 Feb;16(2):E61-75.
https://www.doi.org/10.5489/cuaj.7763
http://www.ncbi.nlm.nih.gov/pubmed/35133268?tool=bestpractice.com
[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
[64]National Cancer Comprehensive Network. NCCN clinical practice guidelines in oncology: kidney cancer [internet publication].
https://www.nccn.org/professionals/physician_gls/default.aspx
Age ≤46 years; and/or
Bilateral or multifocal tumors; and/or
First- or second-degree relative with RCC; and/or
Close blood relative with a known pathogenic variant; and/or
Specific histologic characteristics which suggest a hereditary form of RCC (e.g., multifocal papillary histology; hereditary leiomyomatosis-associated RCC, RCC with fumarate hydratase deficiency or other associated histologic features; multiple chromophobe, oncocytoma or oncocytic hybrid; angiomyolipomas of the kidney and one additional tuberous sclerosis complex criterion; succinate dehydrogenase-deficient RCC histology).
These patients are at a significantly greater risk of having hereditary cancer.
Depending on the outcome of the evaluation, referral to a cancer geneticist or a comprehensive clinical care center may be warranted.[17]European Association of Urology. Renal cell carcinoma. 2023 [internet publication].
https://uroweb.org/guideline/renal-cell-carcinoma
Emerging investigations
There are ongoing studies of standard PET scanning (with FDG tracers) for RCC staging. There are also studies looking at PET scanning utilizing new tracers.[2]Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann Oncol. 2019 May;30(5):706-20.
https://www.annalsofoncology.org/article/S0923-7534(19)31157-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/30788497?tool=bestpractice.com
[66]Karivedu V, Jain AL, Eluvathingal TJ, et al. Role of positron emission tomography imaging in metabolically active renal cell carcinoma. Curr Urol Rep. 2019 Aug 29;20(10):56.
http://www.ncbi.nlm.nih.gov/pubmed/31468240?tool=bestpractice.com