Approach
Patients with recent-onset atrial flutter generally present with palpitations, fatigue, light-headedness, chest pain, and/or dyspnea. In addition, exercise intolerance, worsening heart failure symptoms, and pulmonary complaints can also occur. Less commonly, hypotension, syncope, or embolic events can be the presenting symptoms.[4] The history should be directed at identifying the onset, frequency, and duration, and the presence of structural heart disease or precipitating cause.
History
In approximately 60% of patients, atrial flutter occurs as part of an acute disease process, and resolves with that process.[5] Identifying that underlying cause or trigger is therefore central to management. The history should establish whether there are any concurrent symptoms of an acute disease process, such as fever and cough in the case of pneumonia. A thorough past medical history should identify whether there is a history of any risk factors:
Hypertensive heart disease
Heart failure
Asthma
COPD
Hyperthyroidism
Mitral or tricuspid valve disease
Atrial fibrillation
Structural heart disease, such as hypertrophic cardiomyopathy or congenital heart disease
Recent cardiac or thoracic procedures, including ablation
Prior myocardial infarction (MI) or pulmonary embolism or other pathology that can cause atrial dilation
Diabetes.
A drug history will reveal whether the patient is taking antiarrhythmics for chronic suppression of atrial fibrillation such as class Ic drugs (flecainide and propafenone) or class Ia (disopyramide, procainamide, quinidine) and amiodarone.[7][8][20] Digitalis drugs (e.g., digoxin) are also known to be a risk factor for atrial flutter.
Physical examination
The pulse in a patient with atrial flutter may be regular or irregularly irregular. On examining the jugular venous pressure, jugular venous pulsations with rapid flutter waves may be seen. Manifestations of the underlying cause should be sought through a thorough physical exam. Wheezing, rales, and hyperinflation suggest lung disease. Murmurs or rubs on auscultation suggest valvular disease, pericarditis, or congenital heart disease. Signs of hyperthyroidism may be present, such as tachycardia, fine tremor, goitre with or without nodules, palmar erythema, and hair thinning. Blood pressure should be taken and scars from recent cardiac or thoracic surgery looked for. These may suggest underlying conditions that may complicate therapy.
Investigations
The ECG pattern may fluctuate between atrial flutter and atrial fibrillation. The ECG is diagnostic:
In the typical form (counterclockwise atrial flutter): negatively directed saw-tooth atrial deflections (f waves) in leads II, III, and aVF, and positive deflections in V1 with atrial rates of 240 to 320 bpm.
Typically there is 2:1 atrioventricular (AV) block and the characteristic ventricular rate is 150 bpm.
Variable block may occur leading to an irregular rate.
In the reverse typical form (clockwise isthmus-dependent flutter): positive flutter waves in leads II, III, and aVF, and negative flutter waves in lead V1.
Atypical flutter has an ECG pattern of continuous undulation of the atrial complex, not meeting criteria for typical or reverse typical flutter, with atrial rates >240 bpm.[3][4]
[Figure caption and citation for the preceding image starts]: Typical atrial flutter with variable (3 to 4:1) blockFrom the collection of Dr K.C. Wu [Citation ends].
 [Figure caption and citation for the preceding image starts]: Atrial fibrillationFrom the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Atrial fibrillationFrom the collection of Dr K.C. Wu [Citation ends].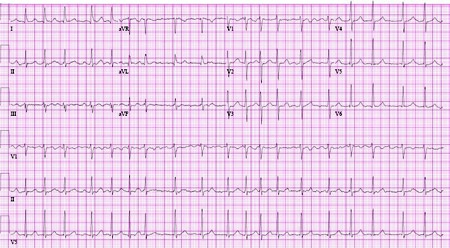 [Figure caption and citation for the preceding image starts]: Close-up images of leads V1, II, III, aVF demonstrating the features of typical atrial flutter: positive saw-tooth deflections in lead V1 and negative deflections in leads II, III, aVF (arrows)From the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Close-up images of leads V1, II, III, aVF demonstrating the features of typical atrial flutter: positive saw-tooth deflections in lead V1 and negative deflections in leads II, III, aVF (arrows)From the collection of Dr K.C. Wu [Citation ends]. [Figure caption and citation for the preceding image starts]: Reverse typical atrial flutterFrom: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Reverse typical atrial flutterFrom: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].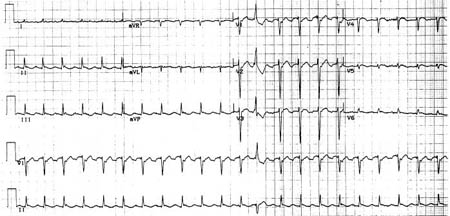 [Figure caption and citation for the preceding image starts]: Selected leads from a patient with reverse typical atrial flutter confirmed at electrophysiologic study. The atrial deflections are negative in lead V1 and positive in leads II, III, aVF (arrows)Adapted from: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Selected leads from a patient with reverse typical atrial flutter confirmed at electrophysiologic study. The atrial deflections are negative in lead V1 and positive in leads II, III, aVF (arrows)Adapted from: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].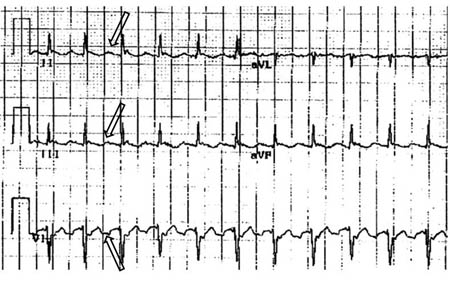 [Figure caption and citation for the preceding image starts]: Atypical flutter with right bundle branch blockFrom the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Atypical flutter with right bundle branch blockFrom the collection of Dr K.C. Wu [Citation ends]. [Figure caption and citation for the preceding image starts]: Close up of leads II, III, V1 showing the continuously undulating pattern of atrial deflections not fitting the criteria for typical or reverse typical atrial flutterFrom the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Close up of leads II, III, V1 showing the continuously undulating pattern of atrial deflections not fitting the criteria for typical or reverse typical atrial flutterFrom the collection of Dr K.C. Wu [Citation ends].
Electrolyte abnormalities are generally not the sole cause of atrial flutter, but imbalances should be checked and corrected. Thyroid function tests should be checked to rule out thyroid disease as an underlying cause. Cardiac enzymes should be checked if acute MI is suspected, and digitalis levels taken if a patient is taking digitalis drugs (e.g., digoxin).
A chest x-ray should be performed and pulmonary function tests should be considered, as atrial flutter is often associated with a known history of, or suggestive presentation for, lung disease. Spiral computed tomography with pulmonary embolism protocol may be considered if pulmonary embolism is suspected.
The transthoracic echocardiogram should be used to detect structural heart disease. Specifically, atrial sizes can be measured and valvular disease, ventricular function, and pericardial disease assessed. Right ventricular systolic pressures can also be measured and indicate the presence or absence of pulmonary hypertension, which can be seen in pulmonary processes.
Electrophysiologic studies are usually performed on patients with recurrent atrial flutter, particularly if antiarrhythmic drug therapy has been ineffective or not tolerated because of adverse effects, if the ventricular rate is difficult to control with drugs, or if atrial flutter persists despite resolution of acute underlying illness. Electrophysiology studies require the input of electrophysiologists and may assist in diagnosis, mapping for the critical isthmus (i.e., the cavotricuspid isthmus), and therapeutic ablation.
An atrial electrogram recording can help visualize flutter waves when diagnosis is not clear. They are recorded by postsurgical epicardial leads, dual chamber pacemaker, or esophageal lead.
Do not use imaging stress tests or coronary CT angiography routinely in the diagnosis of atrial flutter if there are no symptoms or signs of cardiovascular disease.[21]
Use of this content is subject to our disclaimer