Approach
No intrauterine interventions are available for the treatment of omphalocele or gastroschisis. Therapy is therefore undertaken after delivery of the infant, with the goals of temperature maintenance, fluid resuscitation, and preventing additional fluid loss from the abdominal contents with appropriate care of the herniated viscera, paying particular attention to the preservation of its blood supply. Prevention of intestinal ischemia and infarction in gastroschisis is achieved with surgical closure of the defect. Some centers may use prophylactic antibiotics, but antibiotic treatment is not routine and local protocols should be followed.
Gastroschisis
Gastroschisis is a surgical emergency requiring immediate closure or coverage. In gastroschisis, significant fluid balance changes require neonatal fluid resuscitation and emergent surgical intervention to prevent fluid loss and restore the viscera to the abdominal cavity.
Immediate postnatal management of gastroschisis involves fluid resuscitation and the placing of a sterile covering or a clear bowel bag over the herniated abdominal contents to prevent evaporation, heat loss, and infection. The infant should then be urgently transferred to a neonatal intensive unit (NICU) with specialized pediatric surgical capacity.[32]
Small defects may be treated with primary surgical repair, while larger defects or those with extensive herniation of abdominal contents require a staged approach with placement of the abdominal contents into a suspended silo and gradual reduction into the abdominal cavity. Ventilatory support is often required during this process. Once the abdominal contents have been fully reduced into the abdominal cavity, surgery is performed to close the fascia and skin. Occasionally, reduction of pliable bowel is possible in the neonatal unit without the need for operative repair. Such bedside repair in the neonatal unit depends on the size of the defect and presence of healthy abdominal contents.
Surgery is followed by a trial of a nasogastric tube for decompression of the bowel and total parenteral nutrition while the inflammatory peel resolves.[33] If an atretic (ischemic) segment is present, a small bowel obstruction may develop after enteral feeds, necessitating additional surgical intervention. Infants with gastroschisis are often slow to feed due to the intestinal irritation.[Figure caption and citation for the preceding image starts]: Immediately after delivery, an infant with gastroschisis is placed in a protective bowel bagFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends]. [Figure caption and citation for the preceding image starts]: A staged repair of gastroschisis involves the placement of a silo to reduce contents into the abdomenFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
[Figure caption and citation for the preceding image starts]: A staged repair of gastroschisis involves the placement of a silo to reduce contents into the abdomenFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends]. [Figure caption and citation for the preceding image starts]: Once intestinal contents are fully reduced into the abdomen, closure of the abdominal wall followsFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
[Figure caption and citation for the preceding image starts]: Once intestinal contents are fully reduced into the abdomen, closure of the abdominal wall followsFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].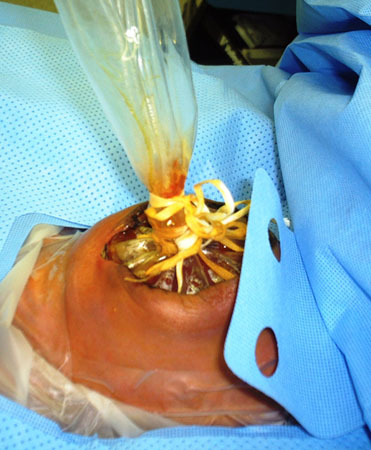
Omphalocele
After delivery, infants with omphalocele should receive appropriate fluid resuscitation. If the membranous sac is not intact, a sterile covering or a clear bowel bag must be placed over the herniated abdominal contents to prevent evaporation, heat loss, and infection.[34] The infant should then be urgently transferred to a NICU with specialized pediatric surgical capacity. A nasogastric tube should be inserted to decompress the bowel.
Surgical repair of omphalocele is elective, unless the membranous sac is ruptured. Defects without rupture of the membranous sac may be allowed to epithelialize, especially if associated anomalies render immediate surgical intervention inappropriately risky. The resultant ventral hernia can be electively repaired at a later date.
If the membranous sac is ruptured, treatment is the same as for gastroschisis. Small defects may be treated with primary surgical repair, while larger defects or those with extensive herniation of abdominal contents require a staged approach with placement of the abdominal contents into a suspended silo and gradual reduction into the abdominal cavity.[35] Ventilatory support is often required during this process. Once the abdominal contents have been fully reduced into the abdominal cavity, the fascia and skin are surgically closed. Surgery is followed by a trial of a nasogastric tube for decompression of the bowel and total parenteral nutrition while the inflammatory peel resolves.[Figure caption and citation for the preceding image starts]: The abdominal wall defect in omphalocele is covered with a synthetic membraneFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends]. [Figure caption and citation for the preceding image starts]: This ruptured omphalocele is similar in appearance to gastroschisisFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
[Figure caption and citation for the preceding image starts]: This ruptured omphalocele is similar in appearance to gastroschisisFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].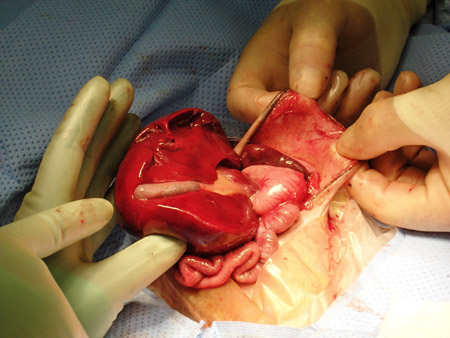 [Figure caption and citation for the preceding image starts]: A ventral hernia results from synthetic wall closure of the omphaloceleFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
[Figure caption and citation for the preceding image starts]: A ventral hernia results from synthetic wall closure of the omphaloceleFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends]. [Figure caption and citation for the preceding image starts]: The ventral hernia is repaired in a 6-year-old girl born with omphaloceleFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
[Figure caption and citation for the preceding image starts]: The ventral hernia is repaired in a 6-year-old girl born with omphaloceleFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].
Use of this content is subject to our disclaimer