Case history
Case history #1
A 22-year-old woman presented to her primary care practitioner with a swelling in her right axilla. The patient noticed the swelling about 3 weeks ago when it was only a small nodule, but it has continued to grow in size. She has not checked her temperature but reports feeling hot and sweaty at times. She denied any significant past medical history. She works as a computer programmer and denied any recent travel or exposures. Examination showed a 3 cm x 5 cm enlarged lymph node in her right axilla, which was fluctuant and tender. There was no pus point or drainage. The lymph node was excised which showed a granulomatous pattern with macrophages and lymphocytes, but Gram stain, acid fast stain, and fungal stains were negative. Her interferon-gamma release assays (for tuberculosis) were negative. The patient was referred to an infectious disease clinic. On further enquiry, the patient reported having a cat at home with which she plays quite often, but does not remember any obvious cat bite or scratch.
Case history #2
A 13-year-old boy was admitted with intermittent high-grade fevers and headache of 2 weeks' duration. He complained of retro-orbital headache, neck stiffness, photophobia, nausea with projectile vomiting, and chills and rigors with fever, mainly in the late evenings. He also had backache for the past 5 days and about 3.6 kg weight loss in 2 weeks. The patient had hamsters as pets, and his friend had recently acquired a new kitten. On examination, he had a fever of 101.9°F (39°C), along with mild tachycardia (pulse rate of 110 bpm). He also had tenderness over his back in the thoracolumbar paraspinal area, but he did not have point tenderness over the vertebrae. A malar rash was present and dermographism was noticed on his skin.
Other presentations
Bartonella henselae may present as fever of unknown origin (FUO), and in one study was the third leading cause of FUO in children.[14]B henselae and B quintana may also present as culture-negative endocarditis, and they account for about 3% of cases of endocarditis.[15] Immunocompetent children may present with hepatosplenic micro-abscesses secondary to B henselae infection, whereas immunocompromised patients present with peliosis hepatis, characterized by dilated capillaries and blood-filled cavernous spaces in the liver. Both conditions manifest with fever, chills, gastrointestinal symptoms, and hepatosplenomegaly. Immunocompromised patients with HIV/AIDS may also develop a systemic disease, bacillary angiomatosis, characterized by reddish-brown papular skin lesions mimicking Kaposi sarcoma. Neurologic involvement in the forms of encephalitis, myelitis, retinitis, facial palsy, and peripheral neuritis may also occur in about 2% of patients with B henselae infection. Other, less common clinical manifestations of B henselae include osteomyelitis, arthritis, mediastinal mass, and pleurisy.[Figure caption and citation for the preceding image starts]: MRI abdomen, cat-scratch disease with disseminated infection: multiple small abscesses in liver, microabscesses in spleenFrom the collection of Janak Koirala, MD [Citation ends].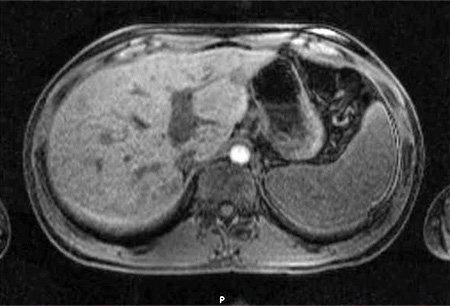
Use of this content is subject to our disclaimer