Case history
Case history #1
A 75-year-old man with type 2 diabetes mellitus presents to the accident and emergency department (A&E) with a 5-day history of abdominal pain that started in the left lower quadrant and was associated with obstipation, nausea and vomiting, and weakness. He has no prior history of abdominal disease or abdominal surgery. The patient is febrile (102.1°F or 39.0°C), tachycardic (heart rate 110 bpm), and hypotensive (systolic blood pressure 80 mmHg). He says he has generalised abdominal pain that is more localised to the left lower quadrant. He has not had any food in the last 24 hours.
Case history #2
A 45-year-old woman has a recent diagnosis of Crohn's disease. Nine days before presentation, she underwent a right hemicolectomy with ileocolic anastomosis for Crohn's disease stricture with small-bowel obstruction. She had an uneventful post-operative course except for intestinal ileus. Her symptoms started 2 days before presentation, when she had to stop eating due to excessive nausea. She now has nausea, anorexia, high-grade fever (104.9°F or 40.0°C), and night sweats. Her abdomen is significantly tender on physical examination, with diffuse tenderness, and she clearly shows peritoneal signs. Her surgical incision has surrounding erythema and is draining purulent fluid.
Other presentations
IAA is commonly related to perforated appendicitis and perforated diverticulitis.[1] It usually presents with fever, abdominal pain, and leukocytosis. IAA can also present without fever or significant abdominal pain, depending on the size, degree of containment, and patient immune system integrity.[3] At the other extreme, the patient may present with clinical signs and symptoms of sepsis or septic shock, especially if very old or young, or immunocompromised. While leukocytosis is usually present, the patient may have leukopenia or even a normal white blood cell count. Primary IAA is extremely rare, but some cases have been reported.[4]
A palpable mass can be the presenting symptom.[5] Untreated IAA can track to the chest, lower extremity/inguinal region, and even scrotum/perineum.[Figure caption and citation for the preceding image starts]: Intra-abdominal abscess with small air bubble, secondary to perforated diverticulitisFrom the collection of Dr Ali F. Mallat and Dr Lena M. Napolitano; used with permission [Citation ends].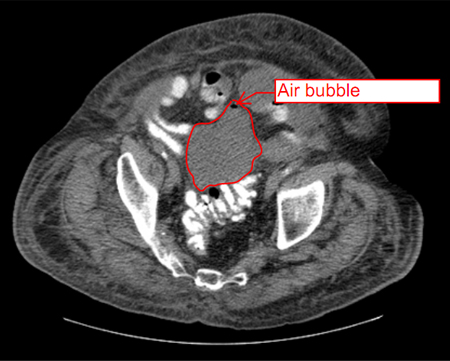
Use of this content is subject to our disclaimer