Investigations
1st investigations to order
FBC
Test
A marked leukocytosis is present in virtually all cases of septic cavernous sinus thrombosis (CST). This may help to distinguish between septic and aseptic CST.
Anaemia is not typical of CST, but if present may suggest disseminated intravascular coagulopathy or sickle cell disease.[61]
Result
normal or low Hb; marked polymorphonuclear leukocytosis with septic CST
contrast-enhanced high-resolution CT of head
Test
CT and MRI scan of the head are the primary radiological modalities used to confirm the diagnosis in all patients and are also used to assess causal and concurrent pathology.[45][54] Neither is absolutely sensitive or specific for the diagnosis of CST. Contrast enhanced CT scan is considered superior to MRI for the detection of early clot formation in the cavernous sinuses, whereas MRI is superior for the rest of the dural venous sinuses.[57]
CT is performed optimally using a dynamic-scanning technique using a bolus injection and continuous infusion of contrast and with scanning in narrow section intervals (less than 3 mm), performing axial and coronal sections.[62]
Angiographic extensions of CT may also be performed.[Figure caption and citation for the preceding image starts]: Sagittal CT scan of the head demonstrating an enlarged, tubular right superior ophthalmic veinJones RG, Arnold B. Sudden onset proptosis secondary to cavernous sinus thrombosis from underlying mandibular dental infection. BMJ Case Rep. 2009;2009. pii: bcr03.2009.1671. Used with permission [Citation ends].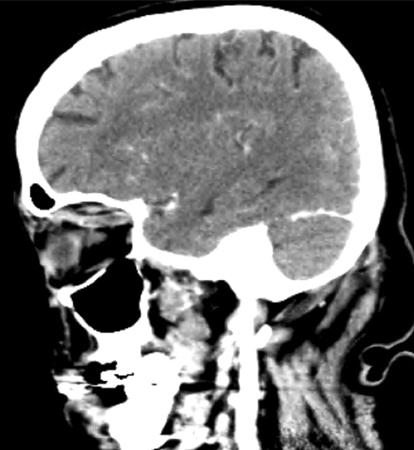 [Figure caption and citation for the preceding image starts]: Post-contrast venous phase CT scan of the head (axial view) showing an enlarged 'S'-shaped right superior ophthalmic vein with associated proptosisJones RG, Arnold B. Sudden onset proptosis secondary to cavernous sinus thrombosis from underlying mandibular dental infection. BMJ Case Rep. 2009;2009. pii: bcr03.2009.1671. Used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Post-contrast venous phase CT scan of the head (axial view) showing an enlarged 'S'-shaped right superior ophthalmic vein with associated proptosisJones RG, Arnold B. Sudden onset proptosis secondary to cavernous sinus thrombosis from underlying mandibular dental infection. BMJ Case Rep. 2009;2009. pii: bcr03.2009.1671. Used with permission [Citation ends]. CT venography may also be useful to confirm the diagnosis in patients with suspected CST.[54][55][56]
CT venography may also be useful to confirm the diagnosis in patients with suspected CST.[54][55][56]
Result
abnormal filling defects together with lateral convexity of the cavernous sinuses
contrast-enhanced MRI of head
Test
MRI and CT scan of the head are the primary radiological modalities used to confirm the diagnosis in all patients and are also used to assess causal and concurrent pathology.[45][54] Neither modality is entirely sensitive or specific for septic CST.
However, contrast enhanced CT scan is considered superior to MRI for the detection of early clot formation in the cavernous sinuses, whereas MRI is superior for the rest of the dural venous sinuses.[57]
May be of greatest value in patients with non-diagnostic CT scans or for evaluating complications involving the pituitary gland or extension of the infection into the brain.
Angiographic extensions of MRI may also be performed. MR venography may also be useful to confirm the diagnosis in patients with suspected CST.[54][55][56] MRV may miss the diagnosis in the dural venous sinuses.[14]
Result
expansion of the cavernous sinuses, convex bowing of lateral walls, increased dural enhancement; sphenoid sinus pathology may be present
blood culture
Test
Bacteriological confirmation of infection can be obtained in the majority of cases of septic CST from the primary infective source, blood cultures, and concurrent suppuration from relevant, accessible sites.
Result
septic CST: may be positive
microscopy and culture of suppurative fluid or tissue from primary infective source
Test
Bacteriological confirmation can be obtained in the majority of cases of septic CST from the primary infective source, blood cultures, and concurrent suppuration from relevant, accessible sites.
Result
septic CST: positive culture of offending organism
antiphospholid and anticardiolipin antibodies
Test
Performed as part of testing for antiphospholipid syndrome. Testing for hypercoagulable states may not be indicated if CST is provoked by strong risk factors e.g., recent history of acute sinusitis or facial infections.[60] Consult a haematologist for specialist advice.
Result
elevated levels indicate a hypercoagulable state
protein S and protein C
Test
Performed as part of testing for a hypercoagulable state. Testing for hypercoagulable states may not be indicated if CST is provoked by strong risk factors e.g., recent history of acute sinusitis or facial infections.[60] Consult a haematologist for specialist advice.
Result
low level or deficiency indicates hypercoagulable state
antithrombin III
Test
Performed as part of testing for a hypercoagulable state. Testing for hypercoagulable states may not be indicated if CST is provoked by strong risk factors e.g., recent history of acute sinusitis or facial infections.[60] Consult a haematologist for specialist advice.
Result
low level or deficiency indicates hypercoagulable state
factor V Leiden
Test
Performed as part of testing for a hypercoagulable state. Testing for hypercoagulable states may not be indicated if CST is provoked by strong risk factors e.g., recent history of acute sinusitis or facial infections.[60] Consult a haematologist for specialist advice.
Result
presence indicates hypercoagulable state
haemoglobin electrophoresis
Test
Only performed in patients with clinical suspicion of sickle cell disease.
Result
haemoglobin S detected in sickle cell disease
Investigations to consider
lumbar puncture with cerebrospinal fluid analysis
Test
May help to exclude meningitis and inform antimicrobial therapy (type and length of therapy) in case a bacterial or fungal agent is isolated.
Result
elevated CSF pressure; inflammatory cells; offending organisms may be detected
Use of this content is subject to our disclaimer