Investigations
1st investigations to order
colonoscopy
Test
The most powerful single diagnostic test, allowing full assessment of the bowel and subsequent polypectomy for histological examination.
Colonoscopy is indicated if there is a suspicion of colorectal polyp or cancer (e.g., anaemia, rectal bleeding, positive faecal immunochemical test, or change in bowel habit). Biopsy or excision of the polyps at endoscopy is important to allow histological examination.
Colonoscopy is superior to CT colonography in the detection of smaller polyps.[24] Colonoscopy is associated with a 6% to 11% miss rate for large (>10 mm) polyps; miss rates are higher for smaller polyps.[25][26]
The risk of perforation is 0.58 per 1000 colonoscopies, and the risk of bleeding is 2.4 per 1000 colonoscopies.[27]
Result
visualisation of presence and site of polyps in colon or rectum
CT colonography
Test
CT colonography (CTC) is a CT technique that uses air insufflation via the rectum and faecal tagging with a radiopaque contrast agent in the bowel-prepared patient.
The site, size, and density of any suspicious lesions (including polyps) are demonstrated by 2D and 3D images. No sedation is required, and the procedure takes around 10 minutes.
CTC has reasonable sensitivity and specificity for detecting larger polyps but may not be as reliable for detecting smaller polyps (<5 mm). The perforation rate of CTC is very low, estimated at 0.04% in one meta-analysis.[39]
The detection of significant polyps prompts endoscopic examination.
[Figure caption and citation for the preceding image starts]: Virtual colonoscopy polypFrom the personal collection of Dr G. Malietzis; used with permission [Citation ends].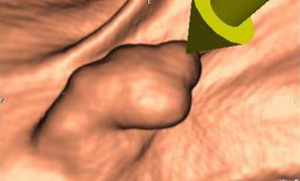
Result
2D and 3D images demonstrate presence of polyps in colon or rectum
chromoendoscopy
Test
Chromoendoscopy aids in the determination of hyperplastic or adenomatous polyps during colonoscopy and is useful in the assessment of flat adenomas. The colonic mucosa is dye-sprayed with indigo carmine and is viewed by magnification endoscopy, which produces different patterns according to the likely histological subtype. Evidence suggests that chromoscopy enhances the detection of neoplasia in the colon and rectum.[29][30][31][32][33]
[ ![]() ]
]
Result
colonic mucosa dye-sprayed with indigo carmine and viewed by magnification endoscopy produces different patterns according to the likely histological subtype
histology
Test
This investigation formally diagnoses a benign polyp, but may not definitively exclude an invasive cancer. A benign diagnosis of an endoscopically malignant lesion should prompt further biopsy. It will define whether the polyp is adenomatous, its morphology (e.g., villous), and degree of dysplasia within the lesion.
Result
neoplastic polyps: adenomas, polypoid adenocarcinomas, lipomas, leiomyomas, and lymphomatous polyps; non-neoplastic polyps: hyperplastic, inflammatory, lymphoid, or hamartomatous; adenomatous polyp morphology may be tubular (containing ≥75% tubular architecture), tubulovillous, villous (containing ≥75% villous architecture), microtubular, serrated, or combined (other than tubulovillous)
Investigations to consider
flexible sigmoidoscopy
Test
Alternative to colonoscopy in patients with a lower risk of proximal polyps, such as younger patients with left-sided symptoms (i.e., bright red rectal bleeding and/or tenesmus). Biopsy or excision of the polyps at endoscopy is important to allow histological examination.
The principal advantage of flexible sigmoidoscopy is the simpler bowel preparation and lack of sedation required for the test; however, it is limited in scope because the examiner cannot inspect the entire colon.
Patients with an identified polyp on flexible sigmoidoscopy should proceed to colonoscopy (unless the presence of proximal polyps has already been excluded by another modality).
Flexible sigmoidoscopy may be performed to resect or take biopsies from polyps in the descending/sigmoid colon or rectum that have been identified using CT colonography.
Result
visualisation of presence and site of left-sided polyps in descending or sigmoid colon or in rectum
Emerging tests
virtual chromoendoscopy techniques
Test
Virtual chromoendoscopy techniques such as narrow band imaging, flexible spectral imaging colour enhancement, and i-scan can be used during colonoscopy to determine whether small polyps are adenomatous or hyperplastic, thus removing the need for subsequent histological classification.[34][35][36]
These technologies allow high-contrast imaging of the mucosal surface without using dyes and other equipment. Further research and endoscopic training is required to permit guidance on their optimal use.[34][37][38]
Result
pit patterns and vascular patterns; several types indicate an increased risk of a lesion being neoplastic
artificial intelligence-assisted colonoscopy
Test
Artificial intelligence (AI), in particular deep learning methods, can utilise data driven algorithms from endoscopic images. AI systems may overcome the limitations of the human eye and uniformly increase the adenoma detection rate.
Large scale meta-analyses have reported a significantly enhanced detection rate of colorectal neoplasia through AI assisted colonoscopy.[41][42]
Further studies are needed to evaluate the cost-effectiveness and long-term benefits of AI assisted colonoscopy in reducing colorectal cancer incidence.
Result
detection of polyps in colon or rectum
capsule endoscopy
Test
Capsule endoscopy is an emerging option for the detection of colonic polyps in instances where optical colonoscopy is not appropriate. It is a non-invasive means of colon polyp detection and also enables assessment of the small bowel. However, it necessitates an intensive bowel cleansing regimen. Second generation capsule endoscopy (CCE-2) has a 87% sensitivity and 76% specificity for the detection of colon polyps >6 mm.[43]
Result
non-invasive detection of colonic polyps >6 mm
Use of this content is subject to our disclaimer