Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
manual manipulation
This is performed to reduce swelling and to replace the foreskin over the glans penis.
Before manipulation, a topical analgesic or injection of a local anaesthetic is required. Young boys often require parenteral administration of opioids and sedative agents in addition to local anaesthesia. Acupuncture is a non-pharmacological option for pain management.[17]
Ice, compression, or an osmotic agent may be applied after the anaesthesia.[18]
Ice packs can be applied to the penis after the penis has been wrapped in plastic.
Compression is commonly performed using a gloved hand but can also be achieved by a 2 x 2-inch bandage. The oedematous glans and foreskin should be compressed until swelling is noted to improve. This technique is successful in the majority of boys with paraphimosis.
Osmotic agent (e.g., fine granulated sugar) is applied in liberal amounts, on the principle that fluid flows down a concentration gradient; in this case the hypotonic fluid in the penis flows to the hypertonic agent on the outside of the skin.[20]
Once foreskin swelling has been reduced as much as possible, manual reduction is performed by pulling the phimotic ring while pushing down on the glans.[18][Figure caption and citation for the preceding image starts]: Pre-reduction of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends]. [Figure caption and citation for the preceding image starts]: Process of manual manipulation of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends].
[Figure caption and citation for the preceding image starts]: Process of manual manipulation of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends].
[Figure caption and citation for the preceding image starts]: Diagram illustrating the technique for manual reduction of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
surgical reduction followed by circumcision
This is reserved for patients who fail conservative attempts at reduction.
Although in very infirm and older people this can be performed at the bedside using a penile block (i.e., local anaesthetic plus procedural sedation), in most patients general anaesthesia will be required.
For the dorsal slit procedure, the phimotic ring is incised on the dorsal aspect of the penis until release of the foreskin is identified. [Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends]. [Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
[Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends]. This allows the swelling to subside. The edges are closed using 4-0 chromic suture or similar.
This allows the swelling to subside. The edges are closed using 4-0 chromic suture or similar.
Completion of the circumcision is performed as a second procedure, once the swelling of the foreskin has subsided. [Figure caption and citation for the preceding image starts]: Completed dorsal slit and reduction of the paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].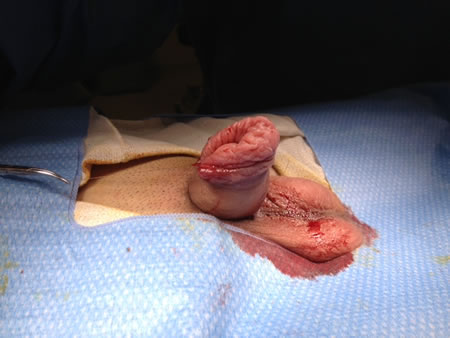
surgical reduction followed by circumcision
Patients with the chronic form of paraphimosis should undergo surgical reduction followed by circumcision as first-line therapy.
Although in very infirm and older people this can be performed at the bedside using a penile block (i.e., local anaesthetic plus procedural sedation), in most patients general anaesthesia will be required.
For the dorsal slit procedure, the phimotic ring is incised on the dorsal aspect of the penis until release of the foreskin is identified. [Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].[Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends]. This allows the swelling to subside. The edges are closed using 4-0 chromic suture or similar.
Completion of the circumcision is performed as a second procedure, once the swelling of the foreskin has subsided. [Figure caption and citation for the preceding image starts]: Completed dorsal slit and reduction of the paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer