Approach
Paraphimosis should be considered a medical emergency, and steps should be taken to rapidly resolve this painful condition to prevent tissue loss.
Careful inspection of the penis should occur to ensure there are no constricting bands or foreign bodies (e.g., piercing studs) present. In the presence of an indwelling catheter, after the reason for its placement has been determined, it should be removed before attempting reduction of the paraphimosis. The catheter can be replaced after successful reduction.
Emergency surgery
Patients with evidence of significant glans penis ischaemia, with necrosis and sloughing of the foreskin and/or glans, require involvement of a consultant in urology. They will require procedural sedation or general anaesthesia, followed by immediate reduction using surgical techniques. Devitalised tissue will require operative debridement.
Acute type without ischaemia and necrosis
Manipulation
The first method of treatment involves manual manipulation of the penis to reduce swelling and to replace the foreskin over the glans penis. Paraphimosis can be extremely painful. Therefore, analgesia should be administered before treatment. The amount of analgesia depends on the patient. Some patients can tolerate topical formulations; others may prefer injection of a local anaesthetic. Young boys often require parenteral administration of opioids and sedative agents in addition to local anaesthetics. The local anaesthetic can be used as a single injection at the dorsal midline of the penis or as a ring block at the base of the penis. One study has utilised acupuncture as a non-pharmacological treatment for pain reduction in paediatric patients undergoing procedures in the accident and emergency department including reduction of paraphimosis.[17][Figure caption and citation for the preceding image starts]: Diagram illustrating the technique for manual reduction of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
Ice, compression, or an osmotic agent is applied after the anaesthesia.[18][19]
Ice packs: these can be applied to the penis (after the penis has been wrapped in plastic) to help reduce swelling.
Compression: this is commonly performed using a gloved hand but can also be achieved by a 2 x 2-inch bandage. The oedematous glans and foreskin should be compressed until swelling is noted to improve. This technique is successful in the majority of boys with paraphimosis.
Osmotic agent: this technique uses the principle that fluid flows down a concentration gradient; in this case the hypotonic fluid in the penis flows to the hypertonic agent on the outside of the skin. The most common agent used is fine granulated sugar, in liberal amounts.[20]
Once foreskin swelling has been reduced as much as possible, manual reduction is performed by pulling the phimotic ring while pushing down on the glans.[18][Figure caption and citation for the preceding image starts]: Pre-reduction of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends]. [Figure caption and citation for the preceding image starts]: Process of manual manipulation of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends].
[Figure caption and citation for the preceding image starts]: Process of manual manipulation of paraphimosisFrom the collection of Dr Michelle Semins and Dr Adam Kern [Citation ends].
Puncture technique
This may be used after failed attempts at reduction using minimally invasive procedures. Perforation of the foreskin at multiple locations (the Dundee technique) allows exudation of the oedematous fluid and reduction in swelling.[13][19][21] After appropriate local analgesia and sedation, multiple punctures are made in the oedematous foreskin using a 22-gauge hypodermic needle. Subsequently, the foreskin is reduced by manual compression and reduction.
Hyaluronidase, a natural protein that causes hydrolysis of hyaluronic acid, an extracellular mucopolysaccharide, may be used to augment the puncture technique.[19][22] Injection of hyaluronidase into the oedematous foreskin leads to degradation of hyaluronic acid and reduction of oedema. Immediate reduction of oedema will be noted and then reduction can be attempted.
Surgical reduction followed by circumcision
This is reserved for patients who fail conservative attempts at reduction. Although in very infirm and older people this can be performed at the bedside using a penile block (i.e., local anaesthetic plus procedural sedation), in most patients general anaesthesia will be required.
For the dorsal slit procedure, the phimotic ring is incised on the dorsal aspect of the penis until release of the foreskin is identified. This allows the swelling to subside. The edges are closed using 4-0 chromic suture or similar. Completion of the circumcision is performed as a second procedure, once the swelling of the foreskin has subsided. [Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
 [Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
[Figure caption and citation for the preceding image starts]: Dorsal slit for management of paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends]. [Figure caption and citation for the preceding image starts]: Completed dorsal slit and reduction of the paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].
[Figure caption and citation for the preceding image starts]: Completed dorsal slit and reduction of the paraphimosisFrom the collection of Dr Ranjiv Mathews [Citation ends].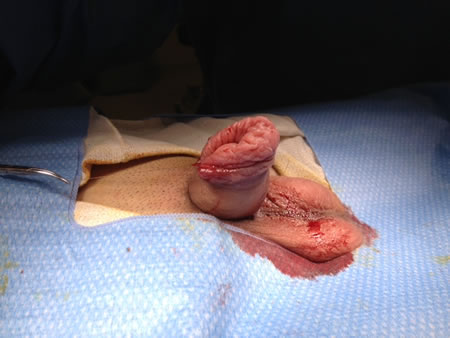
Chronic type without ischaemia and necrosis
These patients should also undergo surgical reduction followed by circumcision.
Use of this content is subject to our disclaimer