Differentials
Vocal cord palsy
SIGNS / SYMPTOMS
Clinical presentation may be similar, although this is often present from birth. Patients have significant feeding problems (choking episodes and recurrent aspiration) and an abnormal or absent cry.
Patients may have a history of birth trauma, Arnold-Chiari malformation, hydrocephalus, or potential for iatrogenic injury, such as recent cardiac surgery.
INVESTIGATIONS
Flexible laryngoscopy demonstrates immobility of one or both vocal cords.
Subglottic stenosis
SIGNS / SYMPTOMS
Clinical presentation may be similar, although stridor may be biphasic rather than inspiratory. Feeding difficulties are usually less severe than in laryngomalacia.
Patients may have a history of previous intubation if stenosis is acquired.
INVESTIGATIONS
Lateral neck radiograph or chest x-ray may demonstrate subglottic narrowing.
Flexible laryngoscopy is usually inadequate for diagnosis.
Rigid laryngobronchoscopy reveals stenosis and allows formal sizing (based on endotracheal tube sizes).[31][Figure caption and citation for the preceding image starts]: Subglottic stenosisFrom the personal teaching collection of Simone J. Boardman, MBBS, FRACS (OHNS) and C. Martin Bailey, BSc, FRCS, FRCSEd [Citation ends].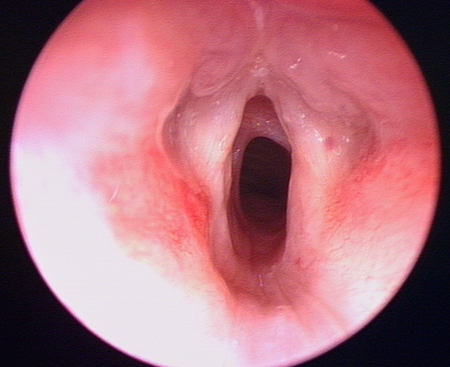
Laryngeal web
SIGNS / SYMPTOMS
Clinical presentation may be similar, although patients have an abnormal, often high-pitched cry.
May be associated with velocardiofacial (Shprintzen's) syndrome.
INVESTIGATIONS
Endoscopic examination of the larynx demonstrates the anterior glottic web. [Figure caption and citation for the preceding image starts]: Glottic webFrom the personal teaching collection of Simone J. Boardman, MBBS, FRACS (OHNS) and C. Martin Bailey, BSc, FRCS, FRCSEd [Citation ends].
Laryngeal cleft
SIGNS / SYMPTOMS
Clinical presentation may be similar, although significant feeding problems (choking episodes and recurrent aspiration) may occur.
INVESTIGATIONS
Endoscopic examination of the larynx demonstrates the defect in the posterior glottis, extending from the interarytenoid region for a variable distance through the cricoid into the tracheo-oesophageal septum. [Figure caption and citation for the preceding image starts]: Laryngeal cleftFrom the personal teaching collection of Simone J. Boardman, MBBS, FRACS (OHNS) and C. Martin Bailey, BSc, FRCS, FRCSEd [Citation ends].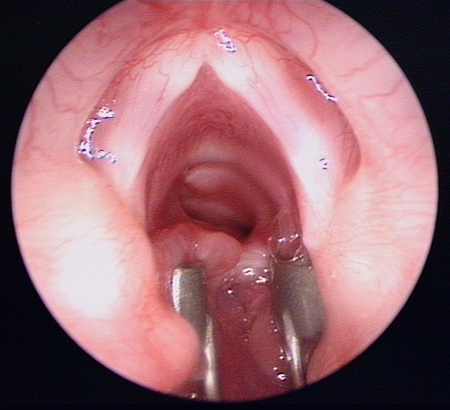
Subglottic haemangioma
SIGNS / SYMPTOMS
Clinical presentation may be similar; 50% of children with a subglottic haemangioma have a concurrent cutaneous lesion.[32]
INVESTIGATIONS
Rigid bronchoscopy allows direct visualisation of the vascular lesion. These lesions typically involve the posterolateral aspect of the subglottis; may be unilateral, bilateral, or circumferential.
Laryngeal or vallecular cyst
SIGNS / SYMPTOMS
Clinical presentation may be similar but typically is present from birth.
May be exacerbated by supine posture and, in the case of vallecular cysts, may be improved with chin lift/jaw thrust. With vallecular cysts the cry is usually unaffected, but it may be abnormal with laryngeal cysts.
Large vallecular cysts may sometimes be seen with direct examination of the oropharynx.
INVESTIGATIONS
A lateral x-ray may show a soft tissue density suggesting the presence of a cyst.
Endoscopic examination of the larynx reveals these cysts. [Figure caption and citation for the preceding image starts]: Vallecular cystFrom the personal teaching collection of Simone J. Boardman, MBBS, FRACS (OHNS) and C. Martin Bailey, BSc, FRCS, FRCSEd [Citation ends].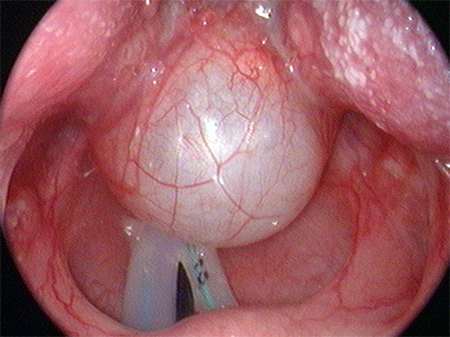
Use of this content is subject to our disclaimer