History and exam
Key diagnostic factors
common
typical age group (<15 years or >25 years)
In endemic areas, where vaccination is uncommon, diphtheria mainly affects children <15 years of age. Where childhood vaccination is commonplace, the epidemiology has shifted to adults (>25 years old) who lack natural exposure to the toxin and do not receive booster vaccinations.[4]
exposure to infected individual
Close contacts of infected individuals should be monitored for evidence of the disease for 7-10 days.[43]
travel from epidemic or endemic regions
Increases the likelihood of diphtheria and is a particularly important risk factor in inadequately immunised individuals.
unvaccinated/incompletely vaccinated individuals
Individuals are at particularly high risk of contracting diphtheria if they have not undergone a full programme of primary vaccination, or have not kept up to date with boosters.[1]
sore throat
Often associated with fever; can progress to difficulty in breathing, with development of pseudomembrane.
Dysphagia, hoarseness, dyspnoea, and a croupy cough are suggestive of laryngeal extension and/or involvement of pharyngeal/laryngeal nerves.[27]
dysphagia or dysphonia
May indicate disease progression and higher risk of respiratory compromise.
dyspnoea
May indicate disease progression and higher risk of respiratory compromise.
croupy cough
May indicate disease progression and higher risk of respiratory compromise.
pseudomembrane formation
Formation of an adherent brown-greyish membrane covering the tonsils, pharynx, and larynx is highly suggestive of diphtheria, and helps to differentiate diphtheria from pyogenic pharyngitis due to Streptococcus pyogenes or Epstein-Barr virus infection.[1]
swelling of the neck
This feature is associated with lymphadenopathy and is characteristic of severe diphtheria.[27] It is usually accompanied by severe malaise, prostration, and stridor.
skin lesions
Cutaneous diphtheria is characterised by a non-progressive, superficial skin infection with a scaling rash or non-healing ulcers covered by grey-brown membranes.[2][3]
Pain, erythema, and exudates are symptoms of cutaneous diphtheria.[5] Lesions often occur at sites of pre-existing wounds or skin conditions.[4]
[Figure caption and citation for the preceding image starts]: Skin lesion caused by the Corynebacterium diphtheriaePublic Health Image Library (PHIL), CDC [Citation ends].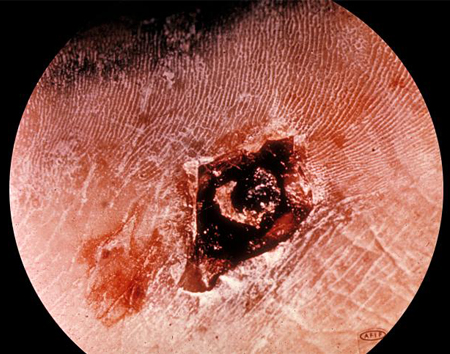
respiratory compromise
Patients may show signs of respiratory compromise at presentation, particularly if the larynx or trachea is affected.
Other diagnostic factors
common
fever
Fever is a common feature, present in over 90% of confirmed diphtheria cases in the 2018-19 outbreak in Cox’s Bazar, Bangladesh.[23] The presenting fever is classically described as low-grade (<39°C [<102°F]), but can be higher.
stridor
Indicative of advanced disease and usually accompanied by severe malaise and prostration.
Risk factors
strong
unvaccinated individuals
Before a vaccine was available, diphtheria was a common cause of illness and death worldwide, but is now rarely reported in countries with high vaccine coverage.[1] Outbreaks of diphtheria are increasingly reported in settings where vaccine coverage is low or immunisation programmes have been interrupted (e.g., in former Soviet states during the dissolution of the USSR, and more recently in Yemen and among Rohingya refugees in Bangladesh).[23][29][30]
inadequately vaccinated individuals
Adults who have not received booster injections and who lack natural exposure to the toxigenic strain of C diphtheriae are more likely to develop the disease than those who are fully vaccinated.[1] Diphtheria outbreaks in Nigeria in 2011 and South Africa in 2015 were associated with low primary vaccination or booster rates.[19][20]
exposure to an infected individual
Person-to-person transmission via respiratory droplets from carriers or sick individuals is the most common form of transmission. Less commonly, transmission can occur from skin lesions of patients with cutaneous diphtheria or via fomites infected with C diphtheriae.[1]
weak
skin breakdown
Skin breakdown from lacerations, burns, or impetigo predisposes to secondary diphtherial infection.[4]
poor hygiene, overcrowding, and poverty
Diphtheria is more common in conditions of poor hygiene and overcrowding, which facilitate disease transmission, especially by respiratory droplets.
Use of this content is subject to our disclaimer