Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
pyloromyotomy
Treatment recommended for ALL patients in selected patient group
Hypovolaemia and electrolyte disturbances must be corrected prior to definitive surgical management.
Pyloromyotomy corrects the gastric outlet obstruction created by the hypertrophied pylorus.[Figure caption and citation for the preceding image starts]: Laparoscopic port placement.From the collection of Dr Jeffrey S. Upperman; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Laparoscopic knife pyloric incisionFrom the collection of Dr Jeffrey S. Upperman; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Laparoscopic knife pyloric incisionFrom the collection of Dr Jeffrey S. Upperman; used with permission [Citation ends].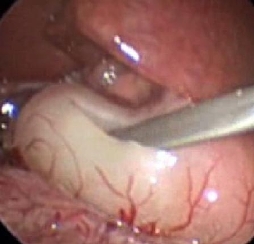 [Figure caption and citation for the preceding image starts]: Muscle-splitting manoeuvreFrom the collection of Dr Jeffrey S. Upperman; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Muscle-splitting manoeuvreFrom the collection of Dr Jeffrey S. Upperman; used with permission [Citation ends].
Laparoscopic and open techniques have been reported to have similar risks, although the laparoscopic approach may increase the risk of mucosal perforation (RR 1.60, 95% CI 0.49 to 5.26), and incomplete pyloromyotomy (RR 7.37, 95% CI 0.92 to 59.11), compared with the open approach.[60][61][62][63][64]
Laparoscopic pyloromyotomy was associated with shorter postoperative recovery time and fewer analgesia requirements than open pyloromyotomy in one large, multicentre international trial.[66]
In centres where laparoscopic surgery is readily performed, it may be the preferred approach.
As most infants with pyloric stenosis are otherwise healthy, there is no preference to perform open versus laparoscopic pyloromyotomy in different patient subsets based on comorbidities.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer