Approach
History and characteristic examination findings are often sufficient to diagnose cutaneous lichen planus. Skin biopsy may be useful to confirm the diagnosis and is often required in more atypical presentations.[46][47] In all cases, it is important to consider the possibility of the eruption being drug induced.[48]
History
Cutaneous LP typically presents with the spontaneous development of intensely pruritic lesions on the flexor wrists, ankles, trunk, and extremities.[2] Patients with oral or genital LP may complain of painful or asymptomatic erosions or ulceration, and those with lichen planopilaris (LP of the scalp) may present with alopecia.[5][6] Symptoms of vulvar LP commonly include dyspareunia, burning, soreness, itching, and increased vaginal discharge.[28] Some patients may present with nail deformity as a single symptom or in combination with other presentations.[7]
Hepatitis C infection or risk factors such as the presence of psychosocial stress should be considered.[42][44]
Consider correlations between lesion onset and initiation of any LP-associated drugs; the most frequently associated drugs include ACE inhibitors, thiazide diuretics, antimalarials, beta-blockers, gold salts, penicillamine, immune checkpoint inhibitors, tyrosine kinase inhibitors, and tumour necrosis factor (TNF)-alpha antagonists. Other drugs have been associated with lichenoid eruptions of the oral mucosa (e.g., allopurinol, ketoconazole, non-steroidal anti-inflammatory drugs [NSAIDs], anticonvulsants, antiretrovirals).[34][45] Certain vaccinations have also been associated with LP (e.g., influenza, coronavirus disease 2019 [COVID-19], hepatitis B).[16][17][18]
Physical examination
Cutaneous
Classically there are violaceous, polygonal papules and plaques. Although these are very pruritic, excoriations are rarely observed. An overlying white lacy network (Wickham's striae), that can be seen with the naked eye, is a characteristic physical sign.[49] Lesions are most commonly found on the flexor wrists and ankles but also on the trunk and extremities.
Bullae that occur in bullous forms of cutaneous LP usually involve previous lesions and not otherwise normal appearing skin. However, LP pemphigoides, an overlap condition between LP and a group of sub-epidermal blistering diseases, presents as tense bullae on normal skin or skin affected by LP.
Annular forms of LP may clinically resemble granuloma annulare; however, epidermal change, such as scale and Wickham's striae, favours a diagnosis of LP.
A crossover condition of LP and lupus erythematosus has also been described. This may present as LP lesions in a photodistribution (at sites routinely exposed to the sun) with or without other signs of lupus erythematosus.[19][20][Figure caption and citation for the preceding image starts]: Cutaneous lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].

Oral and genital
Classically, white reticulation of buccal mucosa, painful desquamative gingivitis, and tongue erosions are seen in oral disease.[3]
LP of the vulva can be categorised into 3 types: erosive, classic, or hypertrophic.[50]
Characteristic features of erosive vulvar LP include a well-demarcated glazed red macule or patch, which may be edged by a white lacy or raised border, located on the labia minora, vestibule, and/or vagina.[50] Architectural changes, such as adhesions or midline fusion of the labia minora, can occur over time.[28][50][51]
Classic vulvar LP can occur anywhere on vulvar skin as a pink-red, purple-brown, or grey-white plaque or papule with an irregular border.[50]
Hypertrophic LP occurs on vulvar and/or perianal skin as a pink-red or violaceous plaque; these are typically circumferential and ovoid with a rounded border.[50]
Concomitant oral involvement is common (occurring in up to 70%) in patients with erosive vulvovaginal LP.[28][Figure caption and citation for the preceding image starts]: Oral lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
 [Figure caption and citation for the preceding image starts]: Genital lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Genital lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Ungual
Classic nail changes comprise lateral thinning of the nail plate, longitudinal ridging, dorsal pterygium, and scarring. [Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
 [Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
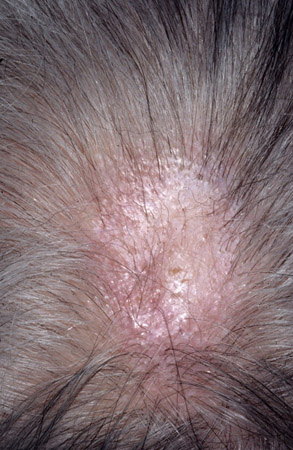
Lichen planopilaris (LP of the scalp)
Follicular keratotic plugs with perifollicular inflammation are seen at onset. Scarring alopecia ensues.[5][6][7][Figure caption and citation for the preceding image starts]: Lichen planopilarisMayo Clinic clinical photographs (used with permission). [Citation ends].
Note that the presence of a single lesion at any site may indicate lichenoid keratosis rather than LP.
Laboratory investigations
History and characteristic examination findings are often sufficient to diagnose cutaneous lichen planus. Serological evidence of hepatitis C may weakly support the diagnosis of LP, but the absence has no diagnostic value.
Histology
Biopsy may be required for diagnostic confirmation. Mucocutaneous biopsy specimens reveal lichenoid infiltrates.[2] Amorphous eosinophilic structures (termed Civatte bodies or colloid bodies) represent necrotic keratinocytes and are generally found at or below the dermal-epidermal junction. Hypergranulosis and hyperkeratosis may also be seen. The silhouettes of epidermal rete ridges may assume saw-toothed appearances.
If histological findings of LP are not present on biopsy, alternate diagnoses or repeat biopsy should be considered if there is strong clinical suspicion or if positive historical factors are present.
Direct immunofluorescence (DIF)
DIF testing is not done in routine practice. However, consider DIF testing on lesional skin or mucosa if previous biopsies were non-diagnostic or if other immune-mediated conditions are suspected. DIF examination of LP skin biopsy specimens reveals necrotic keratinocytes (cytoid bodies) with IgM and linear or shaggy deposition of fibrinogen at the basement membranes.[52]
The sensitivity of these tests is 75%, so absence of these findings does not exclude the diagnosis.[52] DIF is not essential to diagnose LP.
Use of this content is subject to our disclaimer