Aetiology
There are no proven causes, but it is thought that autoimmunity is involved. Hepatitis C may also induce susceptibility by changing cytokine expression in some patient populations.[30] Oral allergens may play a role in oral disease, and meta-analysis suggests a high prevalence of thyroid disease among patients with oral LP.[31][32] Exogenous antigens, such as those found in tattoo ink, may encourage development at tattoo sites.[33] Certain drugs and vaccines have also been associated with LP.[16][17][18][34]
Pathophysiology
Activated T-lymphocytes migrate to dermal-epidermal junctions and induce apoptosis of basal keratinocytes.[1] Although both CD4+ and CD8+ T-lymphocytes are present, the latter predominate in older lesions.[1] It is thought that increased expression of ICAM-1 and Th1 cytokines (including interferon-gamma, TNF-alpha and nuclear factor kappa B [NF-KB] -dependent cytokines) promote apoptosis.[35][36][37][38][39][40][41] Other evidence indicates that neoangiogenesis is an important pathophysiological factor.[41]
Classification
Lesion site
Cutaneous [Figure caption and citation for the preceding image starts]: Cutaneous lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Inverse lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Inverse lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Hypertrophic lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Hypertrophic lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Hypertrophic lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Hypertrophic lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Classically presents with itchy, violaceous, polygonal papules and plaques over the flexor forearms and shins, although other morphologies may be present.[1][2]
Oral [Figure caption and citation for the preceding image starts]: Oral lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
May present with asymptomatic or uncomfortable white, net-like patches or with painful erosions and ulceration.[3]
Genital mucosal [Figure caption and citation for the preceding image starts]: Genital lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
May be associated with pain or pruritus.[4]
Lichen planopilaris [Figure caption and citation for the preceding image starts]: Lichen planopilarisMayo Clinic clinical photographs (used with permission). [Citation ends].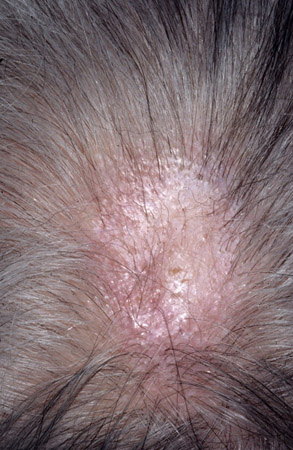
Ungual [Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends]. [Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
[Figure caption and citation for the preceding image starts]: Ungual lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Can cause dorsal pterygium, longitudinal ridging, nail-plate thinning, and distal splitting.[7]
Oesophageal
Rare, can cause dysphagia or odynophagia.[8]
Cutaneous lesion configuration
Blaschkoid [Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].[Figure caption and citation for the preceding image starts]: Blaschkoid lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Zosteriform [Figure caption and citation for the preceding image starts]: Zosteriform lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Lesions following dermatomal lines.[12]
Linear
Inverse [Figure caption and citation for the preceding image starts]: Inverse lichen planusMayo Clinic clinical photographs (used with permission) [Citation ends].
Lesions present in intertriginous areas, such as the groins and axillae. Scale may be absent.[1][2][13]
Cutaneous lesion morphology
Hyper-trophic
Bullous
Actinic
Annular
Lesions in annular configurations.[14]
Atrophic
Atrophic patches that may or may not be associated with hyper-pigmentation.[15]
Erosive
Pigmented
Use of this content is subject to our disclaimer