Aetiology
Tricuspid stenosis (TS) most commonly occurs as a late complication of rheumatic heart disease (RHD). The aetiology of rheumatic TS is still not entirely understood. In nearly all cases, an antecedent case of group A streptococcal pharyngitis is required.
Rare causes of TS include carcinoid syndrome, infective endocarditis, and congenital disease. Carcinoid heart disease usually only occurs in patients whose primary intestinal tumour has metastasised to the liver, at which time a paraneoplastic process causes the tricuspid valve abnormalities.[19]
Infective endocarditis affecting the tricuspid valve can also lead to TS and is most common among those who are intravenous drug abusers or those who have anatomically abnormal tricuspid valves at baseline.
The aetiology of congenital TS is not known, but is thought to be multi-factorial with genetics and environmental factors both playing a role.
Pathophysiology
Anatomical abnormalities of the stenotic tricuspid valve vary by root cause, but generally include fusion of commissural leaflets and foreshortened chordae tendineae.
In rheumatic heart disease (RHD), antibody cross-reactivity between antigens of group A streptococcus (GAS) and host valve tissue leads to an inflammatory response. This ultimately causes progressive fibrin deposition within the valve leaflet and along the cusps. Eventual fusion of leaflet commissures ensues and the chordae tendineae become thickened, fused, and foreshortened, resulting in tricuspid stenosis (TS). GAS-specific immunogenicity, host genetic predisposition, and degree of molecular mimicry are all thought to play a role in the development of acute rheumatic fever (ARF) and subsequent RHD.[6][20]
In carcinoid syndrome, the metastatic carcinoid tumours produce paraneoplastic substances (e.g., serotonin), which are thought to lead to the characteristic endocardial fibrous white plaque formation within the valve leaflets and tricuspid valve chordal apparatus.[19] These fibrous depositions lead to valve distortion, foreshortened leaflets, and the inability of the valve to coapt and open completely, resulting in TS and often tricuspid valve regurgitation.
Infective endocarditis involving the tricuspid valve occurs when certain virulent strains of bacteria circulating in the bloodstream adhere to the surface of the valve. The subsequent inflammatory process results in fibrin, platelet, leukocyte, and red blood cell deposition along the valve leaflet with resulting vegetation formation. Vegetations can then result in further valve thickening, valve perforation, failure of coaptation, and ultimately in a reduced valve orifice and stenosis.
Congenital TS results in some degree of hypoplasia of the right ventricle, pulmonary outflow, and an atrial level shunt. It usually results in annular hypoplasia, incompletely developed leaflets, abnormal chordae tendineae, and dysplastic papillary muscles.
Distortion of the tricuspid valve apparatus and deficiency of the effective valve orifice are pathognomonic findings for all forms of TS, regardless of aetiology. This reduction in the size of the valve orifice results in obstruction of blood flow from the right atrium into the right ventricle during diastole. Because the pressures in the right side of the heart are normally low, a pressure gradient as low as 5 mmHg can result in elevated right atrial pressures, depending on the atrial compliance.[11][21] Chronically elevated right atrial pressures lead to signs and symptoms of systemic venous congestion including prominent jugular venous pulsations with an exaggerated a-wave. In more severe forms of TS, pulmonary blood flow is significantly decreased and cardiac output can become limited, especially at times of increased requirements (i.e., exercise). Right atrial enlargement and hypertrophy can contribute to the development of atrial fibrillation, which significantly exaggerates the symptoms of venous congestion due to the lack of atrial systole.[Figure caption and citation for the preceding image starts]: Congenital tricuspid valve stenosis: 2D transthoracic echocardiogram apical 4 chamber view reveals a small tricuspid valve annulus (dash), RV hypoplasia, and a large atrial septal defect (ASD, arrow)From the personal collection of Martin Bocks; used with permission [Citation ends].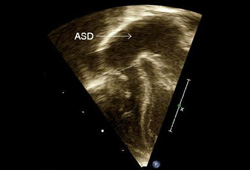
Use of this content is subject to our disclaimer