Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
renal artery stenting + continuation of medical therapy
There are no data supporting routine renal artery stenting in asymptomatic patients in whom RAS is incidentally found.[2]
Renal percutaneous vascular intervention appears to be no better than maximal optimal medical therapy.[45] However, in selected cases, guidelines suggest that renal artery stenting be considered in the following circumstances: refractory hypertension on a multi-drug regimen (≥3 medications); progressive chronic kidney disease; acute kidney injury on ACE inhibitors/angiotensin-II receptor antagonists in patients with congestive heart failure (CHF); recurrent flash pulmonary oedema; bilateral RAS; stenosis of renal artery supplying single functioning kidney; salvage therapy in recent-onset end-stage renal failure; patients with RAS, uncontrolled hypertension, and unstable angina.[3][19][44]
Patient factors that may suggest clinical benefit of revascularisation include a recent onset or exacerbation of hypertension (<1 year), absence of proteinuria, and identifiable activation of the renin-angiotensin system (e.g., hyperreninaemia).[44][Figure caption and citation for the preceding image starts]: Digital subtraction angiography in a patient with significant atherosclerotic left renal artery stenosis. Panel A, prior to stent placement. Panel B, after successful stent deployment. Arrows indicate the site of stenosis and stent placement in their respective panelsCourtesy of Alvaro Alonso, MD and Scott J. Gilbert, MD [Citation ends].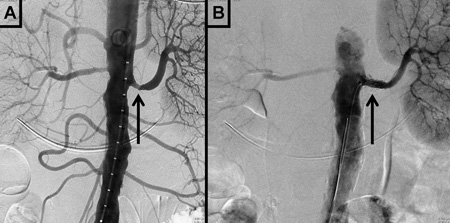
Patients should be referred to a peripheral vascular interventions specialist if revascularisation is considered. Current medical therapy should be continued and maximised. Transient addition of clopidogrel should be considered for dual antiplatelet therapy after the procedure.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer