Aetiology
Atherosclerotic RAS[2][13][Figure caption and citation for the preceding image starts]: Magnetic resonance angiography (3-dimensional volume rendered reconstruction) in a patient with significant bilateral atherosclerotic renal artery stenosis. Arrows indicate proximal bilateral stenosesCourtesy of David J. Sheehan, DO; Radiology Department, University of Massachusetts Medical Center and Medical School [Citation ends].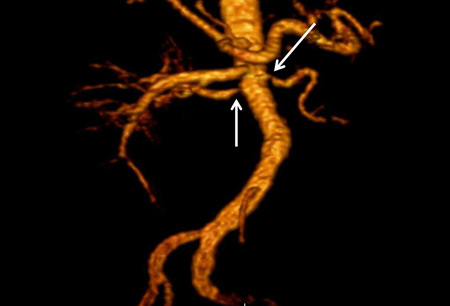
Atherosclerosis
Diabetes mellitus
Dyslipidaemia
Smoking.
Fibromuscular dysplasia[Figure caption and citation for the preceding image starts]: Magnetic resonance angiography (maximum-intensity projection) in a patient with fibromuscular dysplasia of the renal arteries. Arrow indicates the characteristic irregular contour in the right renal arteryCourtesy of Raul Galvez, MD, MPH and Hale Ersoy, MD; Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School [Citation ends].
Smoking.[14]
Other causes of renal artery disease[1][13]
Post-transplant (site of vascular anastomosis)
Renal artery aneurysm
Accessory renal artery
Takayasu's arteritis
Atheroemboli
Thromboemboli
Williams syndrome
Neurofibromatosis
Spontaneous renal artery dissection
Arteriovenous malformations
Arteriovenous fistulas
Trauma
Abdominal radiotherapy
Retroperitoneal fibrosis
Other vasculitis.
Pathophysiology
Activation of the renin-angiotensin system causes increased systemic vascular resistance and sodium retention.
When the stenosis exceeds 50% reduction in vessel diameter, these regulatory mechanisms may fail, leading to worsening kidney function and difficult-to-control hypertension.
Underperfusion of the kidney caused by blood flow obstruction produces adaptive changes in the kidney, including atrophy of tubular cells, fibrosis of the capillary tuft, and intra-renal arterial medial thickening.
Angiotensin II stimulates fibroblast activity, which may lead to fibrosis in the glomerular tuft and in the tubules.
In addition to activation of the renin-angiotensin system, other mechanisms include activation of the sympathetic nervous system, abnormalities in endothelial nitric oxide, endothelin release, and increased oxidative stress.[3]
Hypertension can cause hyalinosis, mesangial cell expansion, and growth factor release resulting in fibrosis.
Bilateral RAS results in volume overload with inappropriately elevated levels of renin.
Usually involves the ostial and proximal third of the renal artery.
Endothelial injury and atherogenesis.
Spontaneous or iatrogenic atheroemboli may further deteriorate kidney function.
Fibromuscular dysplasia:[1][14]
May be focal, occurring in any part of the artery, or multifocal (alternating areas of stenosis and dilation [the so-called ‘string of beads’], which usually occurs in the mid and distal portions of the artery).
Unknown aetiology.
Classification
Use of this content is subject to our disclaimer