Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
laparoscopy
Additional treatment recommended for SOME patients in selected patient group
When to offer surgery is debatable and varies among specialists. It is usually determined by the individual clinician and woman. The patient’s symptoms, preferences and priorities regarding pain and fertility are elements that should be considered.[36] The side effects of hormonal therapy may influence the decision to proceed to surgery. For example, gonadotrophin-releasing hormone agonists and progestogens are not ideal options in adolescents due to the potential impact on bone mineral density at such a critical point in development. Therefore, laparoscopy may be preferred. Furthermore, both progestogens and androgens have bothersome side effects that may result in a preference for surgery.
Conservative surgical management with laparoscopic excision or ablation of visible implants provides effective treatment of pain-related complaints.[Figure caption and citation for the preceding image starts]: Laparoscopic image of endometriotic noduleFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].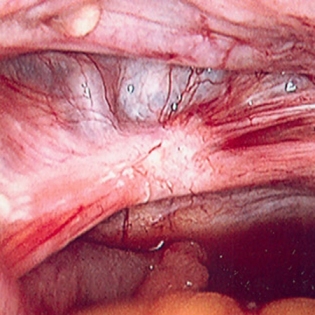 Diagnostic laparoscopy alone may impart a therapeutic response in up to 30% of women.[98] Several studies have established a clear relationship between surgical intervention and reduction of pain in women with endometriosis.
Diagnostic laparoscopy alone may impart a therapeutic response in up to 30% of women.[98] Several studies have established a clear relationship between surgical intervention and reduction of pain in women with endometriosis.
Rectal, bladder, and ureteral injury may occur because of the alterations in normal anatomy. These risks should be discussed prior to surgery. Bowel preparation facilitates these difficult procedures and should be administered to any woman undergoing operative laparoscopy.
Appendectomy should be considered in women undergoing laparoscopic surgery for suspected endometriosis if there is a complaint of right-sided pain and the appendix appears abnormal. Up to 50% of appendiceal specimens will yield abnormal pathology, but the effect on pain and future adverse outcomes is difficult to assess.[101]
laparoscopy
Additional treatment recommended for SOME patients in selected patient group
When to offer surgery is debatable and varies among specialists. It is usually determined by the individual clinician and woman. The patient’s symptoms, preferences and priorities regarding pain and fertility are elements that should be considered.[36] The side effects of hormonal therapy may influence the decision to proceed to surgery. For example, gonadotrophin-releasing hormone agonists and progestogens are not ideal options in adolescents due to the potential impact on bone mineral density at such a critical point in development. Therefore, laparoscopy may be preferred. Furthermore, both progestogens and androgens have bothersome side effects which may result in a preference for surgery.
Conservative surgical management with laparoscopic excision or ablation of visible implants provides effective treatment of pain-related complaints.[Figure caption and citation for the preceding image starts]: Laparoscopic image of endometriotic noduleFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends]. Diagnostic laparoscopy alone may impart a therapeutic response in up to 30% of women.[98] Several studies have established a clear relationship between surgical intervention and reduction of pain in women with endometriosis.
Rectal, bladder, and ureteral injury may occur because of the alterations in normal anatomy. These risks should be discussed prior to surgery. Bowel preparation facilitates these difficult procedures and should be administered to any woman undergoing operative laparoscopy.
Appendectomy should be considered in women undergoing laparoscopic surgery for suspected endometriosis if there is a complaint of right-sided pain and the appendix appears abnormal. Up to 50% of appendiceal specimens will yield abnormal pathology, but the effect on pain and future adverse outcomes is difficult to assess.[101]
laparoscopy
Additional treatment recommended for SOME patients in selected patient group
When to offer surgery is debatable and varies among specialists. It is usually determined by the individual clinician and woman. The patient’s symptoms, preferences and priorities regarding pain and fertility are elements that should be considered.[36] The side effects of hormonal therapy may influence the decision to proceed to surgery. For example, gonadotrophin-releasing hormone agonists and progestogens are not ideal options in adolescents due to the potential impact on bone mineral density at such a critical point in development. Therefore, laparoscopy may be preferred. Furthermore, both progestogens and androgens have bothersome side effects which may result in a preference for surgery.
Conservative surgical management with laparoscopic excision or ablation of visible implants provides effective treatment of pain-related complaints.[Figure caption and citation for the preceding image starts]: Laparoscopic image of endometriotic noduleFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends]. Diagnostic laparoscopy alone may impart a therapeutic response in up to 30% of women.[98] Several studies have established a clear relationship between surgical intervention and reduction of pain in women with endometriosis.
Rectal, bladder, and ureteral injury may occur because of the alterations in normal anatomy. These risks should be discussed prior to surgery. Bowel preparation facilitates these difficult procedures and should be administered to any woman undergoing operative laparoscopy.
Appendectomy should be considered in women undergoing laparoscopic surgery for suspected endometriosis if there is a complaint of right-sided pain and the appendix appears abnormal. Up to 50% of appendiceal specimens will yield abnormal pathology, but the effect on pain and future adverse outcomes is difficult to assess.[101]
surgery
Ovarian endometriomas do not resolve in response to hormonal suppression and, if symptomatic, should be addressed surgically.[Figure caption and citation for the preceding image starts]: Laparoscopic image of ovarian endometriomaFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].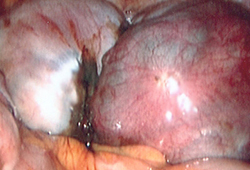
Radical excision of affected areas with restoration of normal anatomy is the preferred method of treating symptomatic women with deep peritoneal disease.[96][97]
NICE advises that 3 months of pre-operative gonadotrophin-releasing hormone (GnRH) agonist treatment should be considered as an adjunct to surgery for deep endometriosis involving the bowel, bladder or ureter.[36]
Improvement in pain may last up to 5 years after surgery, but the risk of re-intervention approaches 50% in women with moderate to severe disease.[98] Less aggressive surgical measures and younger age are predictive of recurrence.[95][99]
For this reason, prolonged hormonal suppression is recommended after surgery for endometriosis.[6]
therapeutic laparoscopy
Additional treatment recommended for SOME patients in selected patient group
The role of surgery is controversial since advanced reproductive technologies successfully treat infertility despite most disease state considerations. However, if symptomatic women without endometrioma or severe deep disease desire fertility, surgery should be offered regardless of age. Women with endometrioma or severe deep disease usually require surgery if pain or large endometrioma (>3 cm) present. Women who fail fertility treatment can be offered surgery, and there is some evidence in support of fertility treatments soon after corrective surgery. One meta-analysis of data from cohort studies found that women who had surgery for deep infiltrating endometriosis before IVF were 2.2 times more likely to have a live birth, compared with unoperated women with deep infiltrating endometriosis who underwent IVF.[109][Figure caption and citation for the preceding image starts]: Laparoscopic image of ovarian endometriomaFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Laparoscopic image of endometriotic noduleFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].
Risk of ovarian failure (reduced number of primordial follicles) after excising endometriomas is approximately 2.4%.[95]
therapeutic laparoscopy
Additional treatment recommended for SOME patients in selected patient group
The role of surgery is controversial since advanced reproductive technologies successfully treat infertility despite most disease state considerations. However, if symptomatic women without endometrioma or severe deep disease desire fertility, surgery should be offered regardless of age. Women with endometrioma or severe deep disease usually require surgery if pain or large endometrioma (>3 cm) present. Women who fail fertility treatment can be offered surgery, and there is some evidence in support of fertility treatments soon after corrective surgery. One meta-analysis of data from cohort studies found that women who had surgery for deep infiltrating endometriosis before IVF were 2.2 times more likely to have a live birth, compared with unoperated women with deep infiltrating endometriosis who underwent IVF.[109][Figure caption and citation for the preceding image starts]: Laparoscopic image of ovarian endometriomaFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Laparoscopic image of endometriotic noduleFrom the collection of Dr Jonathon Solnik; used with permission [Citation ends].
Risk of ovarian failure (reduced number of primordial follicles) after excising endometriomas is approximately 2.4%.[95]
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer