Investigations
1st investigations to order
serum potassium
Test
Order serum potassium in all patients.[12] In an emergency setting, measure potassium using arterial or venous blood gas while waiting for the results from formal laboratory measurement.[1]
There is no universally accepted definition of hyperkalaemia. However, many guidelines use a threshold of serum potassium ≥5.5 mmol/L (≥5.5 mEq/L) and the European Resuscitation Council classification of severity of hyperkalaemia, which is as follows:[1][2][3]
5.5 to 5.9 mmol/L (5.5 to 5.9 mEq/L) - mild
6.0 to 6.4 mmol/L (6.0 to 6.4 mEq/L) - moderate
≥6.5 mmol/L (≥6.5 mEq/L) - severe.
Note that Kidney Disease: Improving Global Outcomes (KDIGO) uses a similar scale but also adds ECG changes to categorise severity; according to the KDIGO scale, mild hyperkalaemia with ECG changes increases the severity level to moderate, and moderate hyperkalaemia with ECG changes increases the severity level to severe.[4]
For more information on severity thresholds, see Criteria.
It is useful to know whether serum or plasma was used for potassium measurement. Plasma potassium concentrations are on average usually 0.1 to 0.4 mmol/L (0.1 to 0.4 mEq/L) lower than serum levels due to release of potassium from platelets during coagulation.[1]
If serum potassium is elevated, exclude pseudohyperkalaemia and spurious hyperkalaemia.[1][2] Assess the probability of these by reviewing the medical history (e.g., for diabetes, heart failure, chronic kidney disease), drug history, and other blood results (e.g., FBC).[2]
Result
mild: 5.5 to 5.9 mmol/L (5.5 to 5.9 mEq/L); moderate: 6.0 to 6.4 mmol/L (6.0 to 6.4 mEq/L); severe: ≥6.5 mmol/L (≥6.5 mEq/L)
12-lead ECG
Test
Obtain an urgent 12-lead ECG in all hospitalised patients with a serum potassium level of ≥6.0 mmol/L (≥6 mEq/L; or use the threshold in your local protocol) to assess for changes associated with hyperkalaemia, which can help to determine the urgency and type of treatment required.[1][2]
Note that the ECG is often normal in hyperkalaemia.[12] If hyperkalaemia-related changes are present, they may correlate with the severity and rate of rise of serum potassium.[1][4] ECG changes may progress from peaked T waves to prolonged PR interval and progressive widening of QRS complex, followed by sine wave patterns, ventricular fibrillation, and asystole.[4]
However, be aware that ECG changes are dependent on a variety of other factors (e.g., concurrent electrolyte abnormalities, acid-base status, prior cardiac injury), and relying on or expecting progressive ECG changes with increasing severity of hyperkalaemia may be misleading and potentially dangerous.[2]
[Figure caption and citation for the preceding image starts]: ECG changes in people with hyperkalaemiaBMJ 2009; 339:b4114. Copyright ©2009 by the BMJ Publishing Group [Citation ends].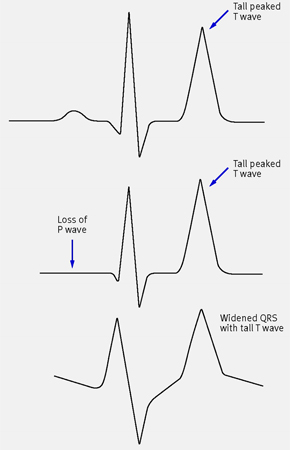
Result
tall peaked T waves, shortened QT interval, ST segment depression, prolonged PR interval, disappearing P wave, widening of QRS (progressive QRS widening may be seen with higher levels of hyperkalaemia), amplified R wave, arrhythmias (atrial fibrillation, bradycardia, ventricular tachycardia)
blood gas
Test
Order if metabolic acidosis is suspected.
In addition, in an emergency setting, measure potassium using arterial or venous blood gas while waiting for the results from formal laboratory measurement.[1]
Result
pH <7.35, low bicarbonate, and/or marked increase in serum anion gap indicates metabolic acidosis
FBC
Test
Order (or review a recent) FBC if you suspect pseudohyperkalaemia (due to potassium released from blood cells during in vitro coagulation) to exclude a haematological disorder.[1] Hyperkalaemia in the setting of significantly elevated white cell count or platelet count with no obvious risk factor for hyperkalaemia (i.e., normal renal function, no ECG changes) indicates pseudohyperkalaemia.
Result
no significant leukocytosis or thrombocytosis
plasma glucose
Test
Always order plasma glucose to exclude hyperglycaemia, which causes cellular redistribution of potassium. Useful in patients with known or suspected diabetes and when diabetic ketoacidosis is likely.
Result
elevated in poorly controlled diabetes or diabetic ketoacidosis
renal chemistry
Test
Always order to check for kidney dysfunction as a cause of hyperkalaemia, and to exclude cellular redistribution of potassium due to metabolic acidosis. Includes, in addition to potassium as discussed above, sodium, chloride, bicarbonate, urea, and creatinine.
Result
creatinine, urea (elevated if kidney dysfunction present); bicarbonate (low if metabolic acidosis present)
serum calcium
Test
Always order serum calcium. Check for hypocalcaemia because this will potentiate the toxicity of hyperkalaemia.[69] Calcium will also be low in rhabdomyolysis, which is a cause of hyperkalaemia.
Result
baseline level; low in rhabdomyolysis
Investigations to consider
uric acid and phosphorus
Test
Order uric acid and phosphorus if there is history of malignancy and/or treatment is being initiated for malignancy to check for tumour lysis syndrome.[70]
Result
elevated in tumour lysis syndrome
creatine kinase
serum digoxin level
Test
Order if the patient is taking digoxin or if suicide is known to have been attempted with digoxin ingestion.
Result
normal or elevated
cortisol and aldosterone levels
Test
Order cortisol and aldosterone levels if you suspect mineralocorticoid deficiency (e.g. primary adrenal insufficiency [Addison's disease]) and other potential causes of hyperkalaemia have been excluded.
Result
normal or low
24-hour urine potassium excretion
Test
Consider 24-hour urine potassium excretion to distinguish renal from extrarenal causes of hyperkalaemia. However, urinary potassium measurements may prove difficult to interpret because multiple factors influence these values independent of level of renal function.
Result
<20 mmol/L (<20 L mEq/L) indicates renal cause of hyperkalaemia; >40 mmol/L (>40 mEq/L) indicates extrarenal cause of hyperkalaemia
plasma and urine potassium and osmolality
Test
Plasma and urine potassium and osmolality is used to calculate transtubular potassium gradient (TTKG). Calculate TTKG if values from 24-hour urine potassium secretion are difficult to interpret. TTKG (TTKG = [K+] urine/(U/P)osm/plasma K+) corrects urinary potassium for changes in osmolality that occur with absorption of water in the collecting duct. TTKG can identify impaired distal tubular secretion of potassium, which can be secondary either to hypoaldosteronism or to aldosterone resistance.
For this formula to be accurate, urine osmolality should be equal to or greater than plasma osmolality and urine sodium should be greater than 25 mmol/L.[71]
Result
<7 suggests impaired distal tubular secretion of potassium; >10 suggests increased intake and intact distal tubular handling of potassium
urine pH
plasma renin activity
Test
Measure plasma renin activity if you suspect pseudohypoaldosteronism.
Result
usually elevated in pseudohypoaldosteronism
Use of this content is subject to our disclaimer