Complications
Severe muscle weakness is a complication of significant hyperkalaemia, commonly presenting as ascending paralysis. This process occurs as a function of depolarisation blockade.[102] Muscle weakness secondary to hyperkalaemia can be of sufficient severity to suppress respiratory effort. The effect of non-depolarising muscle relaxants can be accentuated by concurrent hyperkalaemia. Cardiac arrhythmias often, but not always, accompany muscle paralysis. Urgent reduction in serum potassium values is required to reverse this complication.
Hyperkalaemia has several consequences for the myocardial action potential. The action potential shortens and the myocardium undergoes premature synchronous repolarisation. Conduction velocity increases. These pro-excitatory changes may induce fibrillation or tachyarrhythmias.[96][97]
Life-threatening arrhythmias occur most commonly when factors impairing cellular uptake of potassium co-exist. Presence of hyponatraemia and/or hypocalcaemia can intensify the cardiotoxicity of hyperkalaemia.[69] ECG findings are usually progressive and include first-degree heart block (prolonged PR interval >0.2 s), flattened or absent P waves, tall peaked (tented) T waves (i.e., T wave larger than R wave in more than 1 lead), ST-segment depression, widened QRS (>0.12 s), ventricular tachycardia, bradycardia, and eventually cardiac arrest (pulseless electrical activity, ventricular fibrillation/paroxysmal ventricular tachycardia, asystole).[3] The presence of cardiotoxic ECG changes from hyperkalaemia requires continuous monitoring until serum potassium values have been brought into a safe range and the ECG changes have been corrected.[1][Figure caption and citation for the preceding image starts]: ECG changes in people with hyperkalaemiaBMJ 2009; 339:b4114. Copyright ©2009 by the BMJ Publishing Group [Citation ends].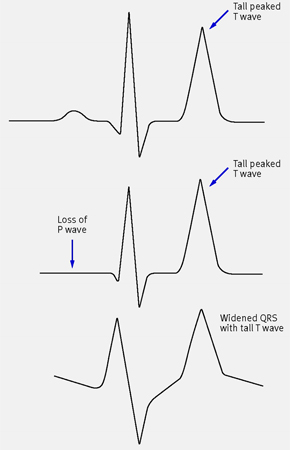
Use of this content is subject to our disclaimer