Choice of investigations for diagnostic work-up of acute dissection is based on the patient’s haemodynamic status, likelihood of aortic dissection, and local availability and expertise.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Consider a formal assessment of the patient’s pre-test probability of aortic dissection - see Pre-test probability of aortic dissection below.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Initially, all patients should have ECG (to rule out ST-elevation myocardial infarction), chest x-ray (if the patient’s clinical status allows), and blood tests (to detect complications of aortic dissection or other differentials).[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[6]Writing Committee Members, Isselbacher EM, Preventza O, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022 Dec 13;80(24):e223-393.
http://www.ncbi.nlm.nih.gov/pubmed/36334952?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
The European Society of Cardiology recommends that transthoracic echocardiography (TTE) should also be used as an initial investigation.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
However, TTE is not widely available in emergency departments in the UK. In practice, computed tomography (CT) may be used initially if the patient is haemodynamically stable and TTE is unavailable or inconclusive.
A protocol of non-enhanced CT, followed by contrast-enhanced CT angiography is recommended.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
The accuracy of CT in the diagnosis of aortic dissection is high with sensitivity and specificity ranging around 98% to100%.[31]Vardhanabhuti V, Nicol E, Morgan-Hughes G, et al. Recommendations for accurate CT diagnosis of suspected acute aortic syndrome (AAS)--on behalf of the British Society of Cardiovascular Imaging (BSCI)/British Society of Cardiovascular CT (BSCCT). Br J Radiol. 2016;89(1061):20150705.
https://www.birpublications.org/doi/full/10.1259/bjr.20150705
http://www.ncbi.nlm.nih.gov/pubmed/26916280?tool=bestpractice.com
If the patient is haemodynamically unstable, seek help from a senior colleague and organise urgent TTE.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[32]Nazerian P, Vanni S, Morello F, et al. Diagnostic performance of focused cardiac ultrasound
performed by emergency physicians for the assessment of ascending aorta dilation and aneurysm. Acad Emerg Med. 2015 May;22(5):536-41.
http://www.ncbi.nlm.nih.gov/pubmed/25899650?tool=bestpractice.com
Confirm the diagnosis using CT.[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
Trans-oesophageal echocardiography (TOE) is an alternative to CT.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
If the patient is haemodynamically stable and you have a high suspicion of dissection, organise urgent CT for definitive diagnosis.[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
TOE and MRI are alternatives.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
Consider other investigations (such as D-dimer, high-sensitivity troponin) initially if you have a low clinical suspicion of aortic dissection.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
If the patient presents with an incidental finding of chronic dissection (such as mediastinal widening or prominent aortic knob on chest x-ray), diagnosis is confirmed by cross-sectional imaging such as contrast-enhanced CT, TOE, or MRI.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
More info: Pre-test probability of aortic dissection
The European Society of Cardiology recommends an assessment of the patient’s pre-test probability of having aortic dissection to determine choice of investigations for diagnostic work-up.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
However, this approach has not been validated and is not always used in practice; check your local hospital protocols.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
The assessment of pre-test probability was proposed by the American College of Cardiology/American Heart Association (AHA) in a 2010 guideline on thoracic aortic disease (no longer available) and is based on the presence of any high-risk features of aortic dissection (see table below).[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Classify the patient’s probability of aortic dissection as:[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Low if they have no high-risk features
Intermediate if they have any single high-risk feature
High if they have two or more high-risk features
[Figure caption and citation for the preceding image starts]: High-risk features of aortic dissectionCreated by the BMJ Knowledge Centre [Citation ends].
There are specific recommendations according to the patient’s pre-test probability. For example, if the patient’s pre-test probability is:[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
High: refer the patient immediately to the surgical team and arrange expedited imaging with either trans-oesophageal echocardiography (TOE), CT, or MRI. TOE is preferred if the patient is haemodynamically unstable.
Intermediate: if you have ruled out alternative causes on ECG and chest x-ray (such as ST-elevation myocardial infarction), arrange expedited imaging with either TOE, CT, or MRI.
Low: investigate other possible causes first. If there is unexplained hypotension or a widened mediastinum on chest x-ray, consider TOE, CT, or MRI based on the individual clinical scenario, but particularly if the patient is older, has risk factors for aortic disease, or has syncope.
ECG
Always perform an ECG in any patient with acute chest pain to rule out ST-elevation myocardial infarction.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
See ST-elevation myocardial infarction.
However, be aware that myocardial ischaemia or infarction may be present in 10% to 15% of patients with aortic dissection, which can mask the diagnosis of dissection.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
This may be due to:
Echocardiography
Organise TTE for all patients with suspected acute aortic dissection, depending on local availability and expertise.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
If the patient is haemodynamically unstable, get help from a senior colleague and organise immediate TTE.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[32]Nazerian P, Vanni S, Morello F, et al. Diagnostic performance of focused cardiac ultrasound
performed by emergency physicians for the assessment of ascending aorta dilation and aneurysm. Acad Emerg Med. 2015 May;22(5):536-41.
http://www.ncbi.nlm.nih.gov/pubmed/25899650?tool=bestpractice.com
Practical tip
In the UK, TTE is not available in many emergency departments and may give poor quality images.[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
In practice, organise CT if TTE is unavailable or inconclusive and the patient is haemodynamically stable.
Consider TOE for definitive diagnosis of acute aortic dissection in addition to TTE, depending on local expertise and availability.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
For type A dissections (ascending), TOE may be performed in the ICU or operating theatre to confirm the diagnosis and better evaluate the aortic valve.
Sensitivity and specificity for TOE are higher than for TTE.
CT and MRI are alternatives, depending on local availability and the patient’s haemodynamic status.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
TOE can also be used to confirm the diagnosis of chronic dissection.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Trans-oesophageal echocardiography (transverse aortic section) showing a circumferential dissection of the ascending aorta in a 30-year-old patient with features of Marfan's syndromeBouzas-Mosquera A, Solla-Buceta M, Fojón-Polanco S. Circumferential aortic dissection. BMJ Case Reports 2009; doi:10.1136/bcr.2007.049908 [Citation ends].
Chest x-ray
Order a chest x-ray for all patients, if the clinical situation allows.[6]Writing Committee Members, Isselbacher EM, Preventza O, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022 Dec 13;80(24):e223-393.
http://www.ncbi.nlm.nih.gov/pubmed/36334952?tool=bestpractice.com
If chest x-ray shows widening of the mediastinum or pleural effusion, this can indicate aortic dissection.[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
Organise further definitive imaging with CT. [14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
TOE and MRI are alternatives.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[33]Miles DR, Boniuk M. Pathogenesis of unilateral glaucoma. A review of 100 cases. Am J Ophthalmol. 1966 Sep;62(3):493-9.
http://www.ncbi.nlm.nih.gov/pubmed/5921996?tool=bestpractice.com
However, if you have a high suspicion of aortic dissection, do not delay definitive imaging for aortic dissection, even if the chest x-ray is normal.[6]Writing Committee Members, Isselbacher EM, Preventza O, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022 Dec 13;80(24):e223-393.
http://www.ncbi.nlm.nih.gov/pubmed/36334952?tool=bestpractice.com
Chest x-ray is of limited value for diagnosis of aortic dissection, particularly if the dissection is confined to the ascending aorta; it is normal in up to 40% of patients with aortic dissection.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
[34]von Kodolitsch Y, Nienaber CA, Dieckmann C, et al. Chest radiography for the diagnosis of acute aortic syndrome. Am J Med. 2004 Jan 15;116(2):73-7.
http://www.ncbi.nlm.nih.gov/pubmed/14715319?tool=bestpractice.com
Chest x-ray may also show other causes of acute chest pain.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Computed tomography (CT)
Use urgent CT as first-line imaging for definitive diagnosis of aortic dissection.[14]Czerny M, Schmidli J, Adler S, et al. Editor's choice - current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) & the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2019 Feb;57(2):165-98.
https://www.doi.org/10.1016/j.ejvs.2018.09.016
http://www.ncbi.nlm.nih.gov/pubmed/30318395?tool=bestpractice.com
TOE and MRI are alternatives, depending on local expertise and availability and the patient’s haemodynamic status.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
In practice, CT may also be used as initial imaging for suspected aortic dissection instead of TTE if this is unavailable or inconclusive, and the patient is haemodynamically stable.
A protocol of non-enhanced CT, followed by contrast-enhanced CT angiography is recommended.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
This should include CT of the chest, abdomen, and pelvis to visualise the extent of the dissection.
[Figure caption and citation for the preceding image starts]: CT scan showing dissecting aneurysm in a 45-year-old patient with Marfan syndrome experiencing chest pain [Citation ends]. [Figure caption and citation for the preceding image starts]: CT of a 71-year-old man showing type II dissecting aneurysm of the ascending aorta. Haematoma around the proximal segment of the ascending aorta (panels A-D) compressed the right pulmonary artery, almost occluding its patency and limiting the perfusion of the reciprocal lung [Citation ends].
[Figure caption and citation for the preceding image starts]: CT of a 71-year-old man showing type II dissecting aneurysm of the ascending aorta. Haematoma around the proximal segment of the ascending aorta (panels A-D) compressed the right pulmonary artery, almost occluding its patency and limiting the perfusion of the reciprocal lung [Citation ends].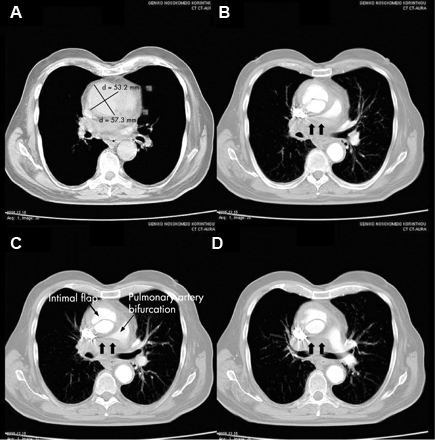
Blood tests
Order a D-dimer (preferably point-of-care) if you have a low clinical suspicion of aortic dissection.[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
Despite a high sensitivity, D-dimer is not recommended as the sole screening tool for acute aortic dissection; while negative D-dimer may be helpful to rule out aortic dissection in a patient with a low clinical suspicion of dissection, a positive D-dimer lacks specificity when used in isolation.[35]Asha SE, Miers JW. A systematic review and meta-analysis of D-dimer as a rule-out test for suspected acute aortic dissection. Ann Emerg Med. 2015 Oct;66(4):368-78.
http://www.annemergmed.com/article/S0196-0644(15)00118-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/25805111?tool=bestpractice.com
[36]Baez AA, Cochon L. Improved rule-out diagnostic gain with a combined aortic dissection detection risk score and D-dimer Bayesian decision support scheme. J Crit Care. 2017 Feb;37:56-9.
http://www.ncbi.nlm.nih.gov/pubmed/27632799?tool=bestpractice.com
However, D-dimer is useful when considering the differential diagnosis (e.g., pulmonary embolism).[18]Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: diagnosis and management, an update. Eur Heart J. 2018 Mar 1;39(9):739-49d.
https://www.doi.org/10.1093/eurheartj/ehx319
http://www.ncbi.nlm.nih.gov/pubmed/29106452?tool=bestpractice.com
[37]Sutherland A, Escano J, Coon TP. D-dimer as the sole screening test for acute aortic dissection: a review of the literature. Ann Emerg Med. 2008 Oct;52(4):339-43.
http://www.ncbi.nlm.nih.gov/pubmed/18819176?tool=bestpractice.com
Request a group and save +/- crossmatch if surgical intervention/transfusion is necessary.
Order the following blood tests in all patients to detect complications of aortic dissection (such as ischaemia) or other differentials:[2]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926.
https://academic.oup.com/eurheartj/article/35/41/2873/407693/2014-ESC-Guidelines-on-the-diagnosis-and-treatment
http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
More info: Biomarkers
Several biomarkers show potential to assist in the diagnosis of aortic dissection, including smooth muscle myosin, calponin, matrix metalloproteinase 8, and soluble elastin fragments. These relate to injury of:
The vascular endothelial or smooth muscle cells (smooth muscle myosin)
The vascular interstitium (calponin, matrix metalloproteinase 8)
The elastic laminae (soluble elastin fragments).
However, none of these have currently been validated and they are not in use in clinical practice.[38]Ranasinghe AM, Bonser RS. Biomarkers in acute aortic dissection and other aortic syndromes. J Am Coll Cardiol. 2010 Nov 2;56(19):1535-41.
http://www.ncbi.nlm.nih.gov/pubmed/21029872?tool=bestpractice.com