Criteria
Atrial flutter is traditionally defined according to the ECG appearance, which shows continuous regular electrical activity, most commonly a saw-tooth pattern.[5]
It is a macro re-entrant atrial tachycardia with constant P wave/flutter morphology with an atrial rate usually >250 beats per minute (bpm).[5] It is distinguishable from focal atrial tachycardia, which has discrete P waves with an intervening isoelectric segment. Focal atrial tachycardia is caused mechanistically by micro re-entry or increased automaticity and generally has atrial rates in the range of 100 to 250 bpm.[2]
Cavotricuspid isthmus-dependent (typical atrial flutter):[2]
Anticlockwise atrial flutter with ECG flutter waves characterised by:[2][5]
Negative deflection in leads II, III, aVF
Positive deflection in lead V1
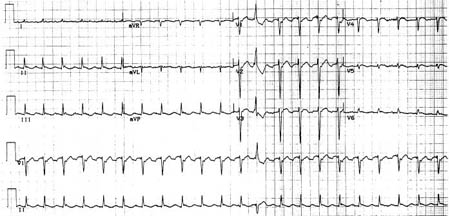
[Figure caption and citation for the preceding image starts]: Typical atrial flutter with variable (3 to 4:1) blockFrom the collection of Dr K.C. Wu [Citation ends].
 [Figure caption and citation for the preceding image starts]: Close-up images of leads V1, II, III, aVF demonstrating the features of typical atrial flutter: positive saw-tooth deflections in lead V1 and negative deflections in leads II, III, aVF (arrows)From the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Close-up images of leads V1, II, III, aVF demonstrating the features of typical atrial flutter: positive saw-tooth deflections in lead V1 and negative deflections in leads II, III, aVF (arrows)From the collection of Dr K.C. Wu [Citation ends].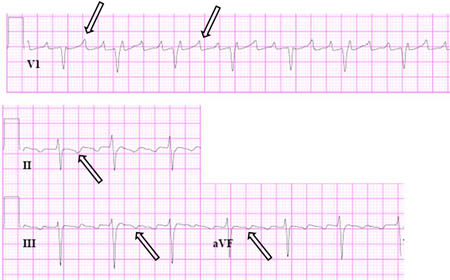
Clockwise atrial flutter (reverse typical atrial flutter) with ECG flutter waves characterised by:
Positive deflection in leads II, III, aVF
Negative deflection in lead V1
[Figure caption and citation for the preceding image starts]: Reverse typical atrial flutterFrom: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Selected leads from a patient with reverse typical atrial flutter confirmed at electrophysiological study. The atrial deflections are negative in lead V1 and positive in leads II, III, aVF (arrows)Adapted from: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Selected leads from a patient with reverse typical atrial flutter confirmed at electrophysiological study. The atrial deflections are negative in lead V1 and positive in leads II, III, aVF (arrows)Adapted from: Waldo AL. Heart. 2000 Aug;84(2):227-32; used with permission [Citation ends].
Non-cavotricuspid isthmus-dependent (atypical atrial flutter):[2]
Re-entry that does not depend upon conduction through the cavotricuspid isthmus
Circuit is typically defined by atrial scars due to prior heart surgery, ablations, or idiopathic causes
Location determines ablation approach and risks
Multiple sites of re-entry may be present
Can occur in both the left and right atria.
[Figure caption and citation for the preceding image starts]: Atypical flutter with right bundle branch blockFrom the collection of Dr K.C. Wu [Citation ends].
 [Figure caption and citation for the preceding image starts]: Close up of leads II, III, V1 showing the continuously undulating pattern of atrial deflections not fitting the criteria for typical or reverse typical atrial flutterFrom the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Close up of leads II, III, V1 showing the continuously undulating pattern of atrial deflections not fitting the criteria for typical or reverse typical atrial flutterFrom the collection of Dr K.C. Wu [Citation ends].
Use of this content is subject to our disclaimer