Stevens-Johnson syndrome and toxic epidermal necrolysis
- Overview
- Theory
- Diagnosis
- Management
- Follow up
- Resources
Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
all patients
urgent evaluation + withdrawal of causative agent
Upon diagnosis, the causative agent should be identified and withdrawn immediately. Usually it will be a new medication prescribed for the patient within the past 2-3 weeks prior to onset of the rash.
Drugs most frequently implicated in SJS/TEN are listed in the aetiology section. See Aetiology.
Patients with SJS/TEN should be assessed in the same way as a patient with cutaneous burns, using a structured approach to evaluate airway, breathing, and circulation. See Cutaneous burns (Diagnosis approach).
Arterial blood gases and oxygen saturation will help determine patient clinical respiratory status.
An immediate assessment of total body surface area (TBSA) involvement is required to assess severity of disease. Various methods can be used, such as the Wallace rule of 9s, Palmer, the Lund-Browder burn estimate chart, or SCORTEN.[55]Lund CC, Browder NC. The estimation of areas of burns. Surg Gynecol Obst. 1944;79:352-8.[57]Wachtel TL, Berry CC, Wachtel EE, et al. The inter-rater reliability of estimating the size of burns from various burn area chart drawings. Burns. 2000 Mar;26(2):156-70. http://www.ncbi.nlm.nih.gov/pubmed/10716359?tool=bestpractice.com Wallace rule of 9s Opens in new window See Diagnosis approach.
[Figure caption and citation for the preceding image starts]: Rule of ninesFrom Dr Sheridan's personal collection [Citation ends].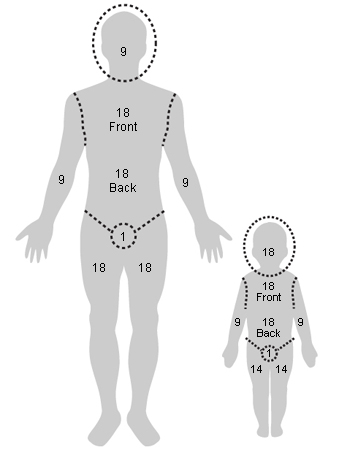 [Figure caption and citation for the preceding image starts]: Lund-Browder diagramFrom Dr Sheridan's personal collection [Citation ends].
[Figure caption and citation for the preceding image starts]: Lund-Browder diagramFrom Dr Sheridan's personal collection [Citation ends].
The greater the percentage of TBSA involved, the greater the fluid requirement.[56]Hettiaratchy S, Papini R. Initial management of a major burn: II - assessment and resuscitation. BMJ. 2004 Jul 10;329(7457):101-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC449823 http://www.ncbi.nlm.nih.gov/pubmed/15242917?tool=bestpractice.com
Consider intubation and early tracheostomy in patients with oral involvement and one of the following: initial body surface area (BSA) 70% or more; progression of BSA involved from day of hospitalisation (DOH) 1 to DOH 3 of ≥15%; underlying neurological diagnosis prevents airway protection; documented airway involvement on direct laryngoscopy.
Evidence suggests that for patients who are intubated, mortality rates increase to over 50%.[54]de Prost N, Mekontso-Dessap A, Valeyrie-Allanore L, et al. Acute respiratory failure in patients with toxic epidermal necrolysis: clinical features and factors associated with mechanical ventilation. Crit Care Med. 2014 Jan;42(1):118-28. http://www.ncbi.nlm.nih.gov/pubmed/23989174?tool=bestpractice.com
Potential oral, ocular, and urogenital involvement should be evaluated as part of the initial assessment of all patients with SJS/TEN.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
venous thromboembolism prophylaxis
Treatment recommended for ALL patients in selected patient group
Provided the patient does not require therapeutic anticoagulation on admission, immobile patients should receive prophylactic low molecular weight heparin (e.g., enoxaparin).[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Mechanical thromboprophylaxis with graduated compression stockings or intermittent pneumatic compression is recommended for acutely ill patients at increased risk of thrombosis who are bleeding or at high risk for major bleeding.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Primary options
enoxaparin: children and adults: consult specialist for guidance on dose
conservative or surgical wound care
Treatment recommended for ALL patients in selected patient group
Wound care can follow either a conservative or surgical approach to debridement and wound care depending on the needs of the individual patient.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
Conservative management (anti-shear strategy) recommends: preserving the detached epidermis as a biological dressing; limiting dressing changes; using an air-fluidised bed and non-adherent dressings; using lysis and drainage of wounds only for patient comfort; cleansing wounds with sterile water or dilute chlorhexidine when dressings are changed; applying an emollient to the whole epidermis to enhance skin barrier function, reduce fluid loss, and encourage re-epithelialisation; considering use of a non-adherent silver-impregnated primary dressing for antibacterial properties, reduced requirement for dressing changes, and improved patient comfort; using secondary absorptive dressings to control exudate.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
The surgical approach for wound care for SJS/TEN patients generally follows practice in burn management: once the surgical debridement of detached epidermis is achieved, wounds are covered with a biological dressing, such as xenograft (pigskin), allograft (cadaver skin), or synthetic dressing.[77]Nizamoglu M, Ward JA, Frew Q, et al. Improving mortality outcomes of Stevens Johnson syndrome/toxic epidermal necrolysis: a regional burns centre experience. Burns. 2018 May;44(3):603-11. http://www.ncbi.nlm.nih.gov/pubmed/29029855?tool=bestpractice.com With healing, consider a non-adherent silver-impregnated dressing for dressing changes and improved patient comfort.
UK guidance recommends that patients should be transferred to a burn unit for surgical debridement and wound care if they have TEN (>30% body surface area epidermal loss) and evidence of the following: clinical deterioration, extension of epidermal detachment, sub-epidermal pus, local sepsis, wound conversion, and/or delayed healing.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
Once the skin has regenerated (after about 2-3 weeks), emollients can be useful to keep it supple and prevent drying out.
analgesia
Treatment recommended for ALL patients in selected patient group
Analgesia should be given based on the severity of symptoms to ensure comfort at rest. Pain level should be evaluated once every 4 hours and assessed at least once daily using a validated pain tool.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Patients will require more pain medication during dressing changes.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
If mild pain is not controlled with paracetamol, an oral opioid such as tramadol should be considered.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Morphine or fentanyl may be necessary for patients with moderate to severe pain scores. Low-dose ketamine an be considered as an alternative or adjuvant therapy for SJS/TEN pain.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Gabapentin and pregabalin both address neuropathic pain and may decrease opioid consumption in both the acute and healing phases for SJS/TEN patients.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Non-steroidal anti-inflammatory drugs should be avoided due to the increased risk of renal or gastric injury.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Primary options
paracetamol: children: consult specialist for guidance on dose; adults (oral): 500-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day; adults <51 kg body weight (intravenous): 15 mg/kg intravenously every 4-6 hours when required, maximum 60 mg/kg/day; adults ≥51 kg body weight (intravenous): 1000 mg intravenously every 4-6 hours when required, maximum 4000 mg/day (3000 mg/day if risk factors for hepatotoxicity)
Secondary options
tramadol: adults: 50-100 mg orally (immediate-release) every 4-6 hours when required, maximum 400 mg/day
Tertiary options
morphine sulfate: children: consult specialist for guidance on dose; adults: 2.5 to 10 mg intravenously/intramuscularly/subcutaneously every 2-6 hours when required, or 0.8 to 10 mg/hour intravenous infusion, or 10-30 mg orally (immediate-release) every 4 hours when required, adjust dose according to response
OR
fentanyl: children and adults: consult specialist for guidance on dose
OR
ketamine: children and adults: consult specialist for guidance on dose
OR
gabapentin: children and adults: consult specialist for guidance on dose
OR
pregabalin: children and adults: consult specialist for guidance on dose
fluid and electrolyte management
Treatment recommended for ALL patients in selected patient group
If a patient is vomiting frequently, dehydration may occur. In addition, depending on the extent of the skin sloughing, the patient may be losing significant amounts of fluids through the denuded skin surface. Electrolyte and fluid balance should be monitored daily.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Patients who can take fluids orally should be encouraged to do so. Otherwise, start intravenous fluids such as lactated Ringer's solution or 0.9% sodium chloride to hydrate the patient. One case series study indicated that approximately 2 mL/kg/% total body surface area may be adequate if there are no other complications.[78]Shiga S, Cartotto R. What are the fluid requirements in toxic epidermal necrolysis? J Burn Care Res. 2010 Jan-Feb;31(1):100-4. http://www.ncbi.nlm.nih.gov/pubmed/20061843?tool=bestpractice.com
Regardless of the calculated quantity of fluid required, the clinical evaluation of patient response is extremely important. Fluid resuscitation is monitored by urine output. It is important that an adult has a urine output of 0.5 mL/kg/hour (30-50 mL/hour) and children weighing <30 kg have an output of 1 mL/kg/hour.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Increase or decrease fluid resuscitation based on the urine output.
nutritional support
Treatment recommended for ALL patients in selected patient group
Oral involvement occurs in the majority of patients with SJS/TEN, resulting in impaired oral intake.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Nutritional support should be administered orally if possible. For patients unable to tolerate oral intake, provide enteral feeding through a nasogastric tube.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Nasogastric tube placement should be avoided in patients with nasopharyngeal mucosa involvement.
Nutritional support of 30-35 kcal/kg should be provided, maintaining close glycaemic control.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com If the patient’s caloric intake is not sufficient with enteral nutrition, it should be supplemented via the parenteral route.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
proton-pump inhibitor
Additional treatment recommended for SOME patients in selected patient group
Patients at high risk of bleeding, and those in whom enteral nutrition cannot be established, should be given a proton-pump inhibitor to prevent stress-related gastritis and intestinal ulceration.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Treatment is usually for up to 14 days; however, patients may require treatment for longer depending on the size of the burn.
Primary options
omeprazole/sodium bicarbonate: children: consult specialist for guidance on dose; adults: 40 mg orally initially, followed by 40 mg in 6-8 hours on day 1, then 40 mg once daily
More omeprazole/sodium bicarbonateDose refers to omeprazole component
oral supportive care
Additional treatment recommended for SOME patients in selected patient group
Oral involvement occurs in the majority of patients with SJS/TEN, resulting in pain, impaired oral intake, and poor oral hygiene. Patients should have an oral examination on presentation and on a daily basis during the acute phase of the illness.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Applying petrolatum ointment on the lips every 2 hours throughout the acute illness is recommended.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
To provide short-term pain relief, oral rinses or sprays with local anaesthetic, anti-inflammatory, and analgesic properties (e.g., viscous lidocaine, benzydamine) should be given, particularly before eating or oral cleansing.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Topical oral coating agents are recommended for pain reduction in patients with oral mucosal involvement.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
The patient’s mouth should be cleaned daily with warm saline mouthwashes or an oral sponge.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
To reduce bacterial colonisation of the mucosa, an antiseptic oral rinse should be used (e.g., diluted chlorhexidine).[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Either a potent topical corticosteroid mouthwash (e.g., dexamethasone) or an ultrapotent topical corticosteroid ointment is recommended during the acute phase of the illness.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ocular supportive care
Additional treatment recommended for SOME patients in selected patient group
All patients manifesting signs and symptoms of SJS/TEN should have an ophthalmological consultation and a full examination upon admission. To preserve vision and reduce complications, ophthalmological follow-up should continue on a daily basis during the acute phase of illness, until it is established that there is no visual deterioration.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com [88]Gregory DG. New grading system and treatment guidelines for the acute ocular manifestations of Stevens-Johnson syndrome. Ophthalmology. 2016 Aug;123(8):1653-8. http://www.ncbi.nlm.nih.gov/pubmed/27297404?tool=bestpractice.com Follow-up should be determined on a case-by-case basis.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Ocular lubricants (drops and ointments) should be administered every 2 hours during the acute stage of illness for patients with ocular involvement.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Daily examination of the entire ocular surface (eyelid skin, eyelid margin, conjunctiva, and cornea) is recommended.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com This should include assessing for forniceal and tarsal conjunctival epithelial defects and early symblephara by everting the eyelids with eyes rotated.
All patients should have fluorescein staining to detect corneal injuries, small foreign objects or particles in the eye, and abnormal tear production.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Resting eyelid position should be assessed for lagophthalmos (incomplete or abnormal closure of the eyelid), especially in unconscious patients, as prevention of corneal exposure is essential.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Amniotic membrane transplantation should be considered during the initial evaluation of any patient thought to have SJS/TEN, and at each follow-up examination during the acute phase.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Coverage of the entire ocular surface with amniotic membrane, together with intensive short-term topical corticosteroids, during the acute phase of SJS and TEN has been shown to be associated with preservation of good visual acuity and an intact ocular surface.[88]Gregory DG. New grading system and treatment guidelines for the acute ocular manifestations of Stevens-Johnson syndrome. Ophthalmology. 2016 Aug;123(8):1653-8. http://www.ncbi.nlm.nih.gov/pubmed/27297404?tool=bestpractice.com
urogenital supportive care
Additional treatment recommended for SOME patients in selected patient group
Urogenital involvement occurs in approximately 70% of women and men with SJS/TEN.[89]Van Batavia JP, Chu DI, Long CJ, et al. Genitourinary involvement and management in children with Stevens-Johnson syndrome and toxic epidermal necrolysis. J Pediatr Urol. 2017 Oct;13(5):490.e1-7. http://www.ncbi.nlm.nih.gov/pubmed/28314701?tool=bestpractice.com [90]Meneux E, Wolkenstein P, Haddad B, et al. Vulvovaginal involvement in toxic epidermal necrolysis: a retrospective study of 40 cases. Obstet Gynecol. 1998 Feb;91(2):283-7. http://www.ncbi.nlm.nih.gov/pubmed/9469290?tool=bestpractice.com This can result in erosions of the scrotum/labia, penis/vulva; dysuria; haematuria; urinary retention; and long-term sequelae such as urethral stenosis and scarring, xerosis, phimosis, dyspareunia, chronic pain, bleeding, sexual dysfunction, infertility, and anxiety.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Examination of the urogenital tract of all patients with SJS/TEN is recommended upon initial assessment and daily during hospitalisation.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com A urinary catheter should be inserted if urogenital involvement is causing significant dysuria/retention.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
The vulvar/urogenital skin/mucosa should be coated with an ointment and/or ointment gauze to help reduce pain and adhesion formation, and facilitate healing, during the acute phase of the disease.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
For women with suspected vaginal involvement, an intravaginal dilator can be used to apply a non-steroidal ointment (e.g., petrolatum jelly), with reapplication as frequently as necessary to maintain barrier protection and/or a high-potency corticosteroid ointment if active inflammation is observed.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227. https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530 http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com [74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com Tapering of the topical corticosteroid use should be based on clinical improvement.
If vaginal candidiasis is suspected, obtain a potassium hydroxide preparation and fungal culture and initiate treatment with a suitable antifungal medication.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Medication can be alternated with oestrogen cream to encourage healing of the vaginal mucosa.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
Intravaginal dilators can be in place for a maximum of 24 hours before replacement.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com If patients are not comfortable using an intravaginal dilator, medication can be applied with a vaginal applicator.
Menstrual suppression may reduce the risk of vaginal adenosis and endometriosis, and can be considered in women with severe genital mucosal involvement.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67. http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
intravenous immunoglobulin
Additional treatment recommended for SOME patients in selected patient group
There are no clear indications regards administration of intravenous immunoglobulin (IVIG); this treatment may be used by some clinicians depending on individual patient presentations.
Some clinicians give IVIG to patients with a rapidly progressing rash involving ≥6% of total body surface area (TBSA). Others only give IVIG when 20% TBSA is affected. There are no definitive randomised controlled trials to guide treatment.
IVIG is reserved for patients who have a rapid progression of their mucocutaneous signs and symptoms; comorbidities also determine the type of treatment that the patient will receive.
For SJS/TEN overlap and TEN patients, many burn centres give IVIG when there is rapid progression of the rash, and when the patient is clinically deemed a candidate.
Particular caution is required in patients with renal impairment.[2]Dodiuk-Gad RP, Chung WH, Valeyrie-Allanore L, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: an update. Am J Clin Dermatol. 2015 Dec;16(6):475-93. http://www.ncbi.nlm.nih.gov/pubmed/26481651?tool=bestpractice.com [81]Enk A, Hadaschik E, Eming R, et al. European guidelines (S1) on the use of high-dose intravenous immunoglobulin in dermatology. J Dtsch Dermatol Ges. 2017 Feb;15(2):228-41. http://www.ncbi.nlm.nih.gov/pubmed/28036140?tool=bestpractice.com
Doses used vary widely and are based on literature case reports, anecdotes, and small series.[44]Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis. Part II: prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol. 2013 Aug;69(2):187. http://www.ncbi.nlm.nih.gov/pubmed/23866879?tool=bestpractice.com [79]Barron SJ, Del Vecchio MT, Aronoff SC. Intravenous immunoglobulin in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis: a meta-analysis with meta-regression of observational studies. Int J Dermatol. 2015 Jan;54(1):108-15. http://www.ncbi.nlm.nih.gov/pubmed/24697283?tool=bestpractice.com [80]Aires DJ, Fraga G, Korentager R, et al. Early treatment with nonsucrose intravenous immunoglobulin in a burn unit reduces toxic epidermal necrolysis mortality. J Drugs Dermatol. 2013 Jun 1;12(6):679-84. http://www.ncbi.nlm.nih.gov/pubmed/23839186?tool=bestpractice.com [81]Enk A, Hadaschik E, Eming R, et al. European guidelines (S1) on the use of high-dose intravenous immunoglobulin in dermatology. J Dtsch Dermatol Ges. 2017 Feb;15(2):228-41. http://www.ncbi.nlm.nih.gov/pubmed/28036140?tool=bestpractice.com
Primary options
normal immunoglobulin human: children and adults: consult specialist for guidance on dose
ciclosporin
Additional treatment recommended for SOME patients in selected patient group
There are no definitive randomised controlled trials to guide treatment. In a retrospective chart review of 71 patients with SJS/TEN, ciclosporin was associated with fewer deaths than expected (standardised mortality ratio 0.43) while intravenous immunoglobulin was associated with excess mortality (standardised mortality ratio 1.43).[82]Kirchhof MG, Miliszewski MA, Sikora S, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014 Nov;71(5):941-7. http://www.ncbi.nlm.nih.gov/pubmed/25087214?tool=bestpractice.com Another study of 16 patients treated with ciclosporin demonstrated a lower mortality rate than predicted by the SCORTEN score.[83]Balai M, Meena M, Mittal A, et al. Cyclosporine in Stevens-Johnson syndrome and toxic epidermal necrolysis: experience from a tertiary care centre of South Rajasthan. Indian Dermatol Online J. 2021 Jan-Feb;12(1):116-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7982025 http://www.ncbi.nlm.nih.gov/pubmed/33768032?tool=bestpractice.com Results from one small (n=29) phase 2 open-label trial suggest that ciclosporin can reduce mortality and the progression of epidermal detachment among patients with SJS/TEN. There was one death in a small study of 12 patients with an average total body surface area of 77% treated with ciclosporin and plasmapheresis.[84]Valeyrie-Allanore L, Wolkenstein P, Brochard L, et al. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010 Oct;163(4):847-53. http://www.ncbi.nlm.nih.gov/pubmed/20500799?tool=bestpractice.com Other meta-analyses suggest that ciclosporin use in epidermal necrolysis is effective in reducing the risk of death.[75]Zimmermann S, Sekula P, Venhoff M, et al. Systemic immunomodulating therapies for Stevens-Johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2017 Jun 1;153(6):514-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5817620 http://www.ncbi.nlm.nih.gov/pubmed/28329382?tool=bestpractice.com [85]Ng QX, De Deyn MLZQ, Venkatanarayanan N, et al. A meta-analysis of cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res. 2018 Mar 28;11:135-42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880515 http://www.ncbi.nlm.nih.gov/pubmed/29636627?tool=bestpractice.com [86]González-Herrada C, Rodríguez-Martín S, Cachafeiro L, et al. Cyclosporine use in epidermal necrolysis is associated with an important mortality reduction: evidence from three different approaches. J Invest Dermatol. 2017 Oct;137(10):2092-100. https://www.jidonline.org/article/S0022-202X(17)31645-7/fulltext http://www.ncbi.nlm.nih.gov/pubmed/28634032?tool=bestpractice.com [87]Roujeau JC, Mockenhaupt M, Guillaume JC, et al. New evidence supporting cyclosporine efficacy in epidermal necrolysis. J Invest Dermatol. 2017 Oct;137(10):2047-9. https://www.jidonline.org/article/S0022-202X(17)32758-6/fulltext http://www.ncbi.nlm.nih.gov/pubmed/28941473?tool=bestpractice.com
Primary options
ciclosporin: children and adults: consult specialist for guidance on dose
physiotherapy and occupational therapy
Additional treatment recommended for SOME patients in selected patient group
Patients can develop limitations in mobility with decreased strength. Arrange for daily exercises within the patient's capability with a physiotherapist and, if needed, an occupational therapist.[44]Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis. Part II: prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol. 2013 Aug;69(2):187. http://www.ncbi.nlm.nih.gov/pubmed/23866879?tool=bestpractice.com
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer