Investigations
1st investigations to order
serum 17-hydroxyprogesterone
Test
Performed to exclude 21-hydroxylase-deficient non-classic (adult-onset) adrenal hyperplasia (NCAH).
If the value is between 6 and 24 nmol/L (200 and 800 ng/dL), a level obtained 60 minutes after adrenocorticotrophic hormone stimulation is indicated to rule out the disorder.[71] Stimulated values >30 nmol/L (1000 ng/dL) (usually >45 nmol/L [1500 ng/dL]) occur when the woman has NCAH.
Result
>24 nmol/L (>800 ng/dL) indicates adrenal hyperplasia
serum prolactin
Test
This test is performed to exclude hyperprolactinaemia, which may present with oligo- or anovulation.
However, low-level prolactin elevations 870-1304 pmol/L (20-30 ng/mL or 20-30 micrograms/L) are common in polycystic ovary syndrome without associated galactorrhoea or pituitary adenoma on imaging.
Result
elevation may suggest prolactinoma
serum thyroid-stimulating hormone
Test
Active thyroid dysfunction may present with oligo- or anovulation, or irregular and heavy menstrual bleeding.
Result
abnormal in thyroid disease
oral glucose tolerance test
Test
Fasting glucose measurement, followed by glucose measurement 2 hours after administration of 75 g of glucose given orally.
Prevalence of abnormal glucose tolerance (impaired fasting glucose, impaired glucose tolerance or diabetes) is as high as 40% in polycystic ovary syndrome (PCOS).[5] In one meta-analysis, the odds of prevalent impaired glucose tolerance was 3.3, and of prevalent diabetes 2.9, in PCOS.[65]
All women should be screened for impaired glucose tolerance with an oral glucose tolerance test. Those with normal glucose tolerance should be re-screened at least every 2 years. Those with impaired glucose tolerance should be screened annually for type 2 diabetes.[66]
Assessment of insulin resistance/hyperinsulinaemia is problematic, given variability in insulin assays and the need for population-specific normative ranges. However, insulin levels may be measured to give insight into whether insulin resistance is present.
A fasting insulin >69 to 104 pmol/L (10-15 micro-units/mL) may suggest insulin resistance.
During the oral glucose tolerance test, a peak insulin of 695-1042 pmol/L (100-150 micro-units/mL) may indicate mild insulin resistance, 1042-2084 pmol/L (150-300 micro-units/mL) moderate insulin resistance, and >2084 pmol/L (300 micro-units/mL) severe insulin resistance.[67]
Result
fasting glucose level between 5.6 and 6.9 mmol/L (100 and 125 mg/dL) is impaired fasting glucose; impaired glucose tolerance is 2-hour glucose of 7.8 to 11.0 mmol/L (140-199 mg/dL); diabetes is defined as fasting glucose ≥7 mmol/L (126 mg/dL), or 2-hour glucose ≥ 11 mmol/L (200 mg/dL)
fasting lipid panel
Test
Dyslipidaemia is often observed in polycystic ovary syndrome (PCOS).[72][73][74] Assessment of fasting lipids has been advocated for all women with PCOS.[57]
Treatment may be instituted if cardiovascular risk is increased, based on overall evaluation of risk factors.
Result
elevated total cholesterol, LDL-cholesterol, triglycerides; low HDL-cholesterol
Investigations to consider
serum total and free testosterone
Test
Elevation >2 standard deviations above the mean qualifies as a positive test. Many laboratory reference ranges for androgens in women did not carefully exclude women with polycystic ovary syndrome (PCOS).[61][62] Testosterone levels are difficult to measure in women; even assays using liquid chromatography mass spectrometry exhibit poor precision at the low levels characteristically found in women.[60]
Hyper-androgenaemia is present in 60% to 80% of women with PCOS: 70% have elevated free testosterone, 40% have elevated total testosterone, 25% have elevated dehydroepiandrosterone sulfate.[3]
In obese women, sex hormone-binding globulin levels are low, resulting in elevated free testosterone and often normal total testosterone. Androgen level tests should be performed in the follicular phase (in cycling women), in the morning, and at least 3 months after cessation of any hormonal therapies. An exception to these hormonal therapies is a cyclic progestin.[63]
Result
elevated
serum dehydroepiandrosterone sulfate (DHEAS)
Test
May be done if other serum androgens are normal. Elevation >2 standard deviations above the mean qualifies as a positive test. Many laboratory reference ranges for androgens in women did not carefully exclude women with polycystic ovary syndrome (PCOS).[61]
Hyper-androgenaemia is present in 60% to 80% of women with PCOS: 70% have elevated free testosterone, 40% have elevated total testosterone, 25% have elevated DHEAS.[3]
DHEAS levels are the only elevated androgen in 10% of women with PCOS.
The American College of Obstetricians and Gynecologists PCOS guideline suggests evaluating DHEAS is of little value except in cases of rapid virilisation.[64]
Result
elevated
serum androstenedione
Test
May be done if other serum androgens are normal. Measurement may increase the number of women identified as hyper-androgenaemic by 10%.[3]
Result
elevated
pelvic ultrasound
Test
Polycystic ovaries are present in 75% of women with polycystic ovary syndrome (PCOS), but are also seen in up to 25% of normal women and women with other endocrinopathies such as congenital adrenal hyperplasia, hyperprolactinaemia, or hypothalamic amenorrhoea.[3][Figure caption and citation for the preceding image starts]: Polycystic ovarian ultrasoundFrom the collection of Dr M.O. Goodarzi; used with permission [Citation ends].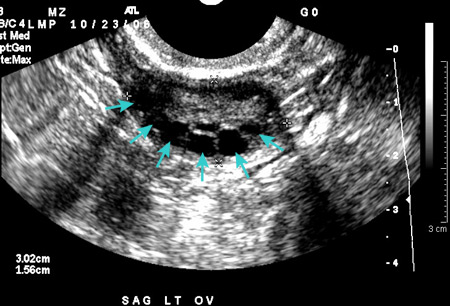
Transvaginal ultrasound, where appropriate, gives higher-resolution images of the ovaries than trans-abdominal ultrasound. Ovarian volume may be estimated as 0.5 x length x width x thickness.[2]
Ultrasound should be done in the early follicular phase (day 3-5) after a spontaneous or progestin-withdrawal-induced menstruation, or randomly in women with infrequent/reduced menstrual bleeding. If evidence of a dominant follicle (>10 mm) or a corpus luteum is seen, the ultrasound should be repeated at the next cycle.[2]
Polycystic ovarian morphology is a risk factor for ovarian hyperstimulation syndrome in women undergoing ovulation induction (with clomifene or gonadotrophins). Therefore, an ultrasound before ovulation induction may be useful.
If endometrial thickening is found, an endometrial biopsy is indicated to determine whether endometrial hyperplasia or cancer is present. Routine ultrasound screening for endometrial thickness is not recommended.[53]
It should be noted that ovarian volume and follicular number decrease with age, so standard criteria may not be applicable to women >40 years of age.[58] Also, multi-follicular ovaries may be observed during puberty, subsiding once the normal menstrual pattern is established.[52]
The International PCOS Network guideline recommends against ultrasound for diagnosis of PCOS in adolescents due to poor specificity.[53]
Result
≥20 follicles in each ovary measuring 2-9 mm in diameter, and/or increased ovarian volume (≥10 mL) in either or both ovaries (using endovaginal ultrasound at 8 MHz); endometrial lining >5 to 7 mm in thickness indicates endometrial thickening. If using older ultrasound technology or transabdominal ultrasound, focus on ovarian volume ≥10 mL in either ovary as a positive test
serum anti-Mullerian hormone
Test
May be considered as an alternative to pelvic ultrasound in adults. Not recommended for diagnosis of polycystic ovary syndrome (PCOS) in adolescents due to poor specificity in this age group.[53]
One meta-analysis reported a pooled sensitivity of 0.78 (95% CI: 0.74 to 0.81) and a specificity of 0.87 (95% CI: 0.84 to 0.90) for diagnosing PCOS.[59] However, there was substantial heterogeneity between studies and optimal cut-off values have not been defined.[59]
Result
elevated
basal body temperature monitoring
Test
Up to 20% of women suspected of having polycystic ovary syndrome report regular menses.[3] In such cases, investigation to document anovulation may be indicated.
Result
biphasic pattern indicates ovulation has occurred; flat pattern indicates anovulation
luteal phase progesterone measurement
Test
Performed on day 20-24 of the menstrual cycle.
Up to 20% of women suspected of having polycystic ovary syndrome report regular menses.[3] In such cases, investigation to document anovulation may be indicated.
Result
>6.4 to 25.4 nmol/L (>2-8 ng/mL) indicates ovulation has occurred
serum LH and follicle-stimulating hormone (FSH)
Test
LH pulses are abnormally elevated (frequency and amplitude), leading to increased serum LH levels and LH/FSH ratio >3 in only two-thirds of women with polycystic ovary syndrome (PCOS).
LH/FSH ratio is elevated more often in lean women. This ratio is helpful only if positive, and is not diagnostic.
Checking LH and FSH is also useful to rule out hypothalamic amenorrhoea (levels low) or perimenopause/ovarian failure (levels high).
Result
LH/FSH ratio >3 suggests PCOS
haemoglobin A1c or fasting plasma glucose
Test
Given the high frequency of insulin resistance and metabolic syndrome in polycystic ovary syndrome, testing should be performed in all women at diagnosis to evaluate metabolic risk factors.[53][64]
Fasting plasma glucose or haemoglobin A1c are less accurate than oral glucose tolerance testing, but may be considered as second-line alternatives if an oral glucose tolerance test cannot be performed.[53][68]
Result
fasting glucose level between 5.6 and 6.9 mmol/L (100 and 125 mg/dL) is impaired fasting glucose; haemoglobin A1c of 39-47 mmol/mol (5.7% to 6.4%) is consistent with prediabetes; diabetes is defined as fasting glucose ≥7 mmol/L (≥126 mg/dL), or haemoglobin A1c ≥48 mmol/mol (≥6.5%)
Use of this content is subject to our disclaimer