Prognosis
Mortality in spina bifida has been reduced immensely by surgical advancements including early closure of the cele within the first 48 hours and shunting of hydrocephalus. The second major influence on survival for this population has been clean intermittent bladder catheterisation every 4 to 6 hours, protecting the kidneys from hydronephrosis and reducing risk of infection. Since survival has improved dramatically with these treatments (over 75% to 85% reaching adulthood), rehabilitation has become a key component to achieve full participation in life activities. It is important also to keep in mind the social determinants of health. Children with birth defects born to non-Hispanic black and Hispanic mothers carry a greater risk of mortality well into childhood. Understanding survival differences among racial/ethnic groups provides important information for policy development and service planning.[134]
Infancy
All infants affected by anencephaly are stillborn or die shortly after birth. For infants born with myelomeningocele, the prognosis varies depending upon availability of treatment and societal attitudes regarding disability. For example, death rates in rural China approach 100%, whereas in the Netherlands the rate is 35%.[135] In the US, death in infancy is rare and typically due to neurosurgical complications of shunted hydrocephalus and/or the Chiari malformation. A small subset of patients who have severe oromotor dysfunction and airway compromise due to the Chiari malformation are medically fragile and at significant risk for sudden death.[136][137][Figure caption and citation for the preceding image starts]: Brain MRI scan showing Chiari malformationFrom the collection of Dr Nienke P. Dosa; used with permission [Citation ends].
Childhood
In general, prognosis is dependent on neurological outcome and especially deterioration due to shunt obstruction or malfunction, or tethered cord with neurological decline. Renal damage can also affect prognosis, such that dialysis leads to poorer functional outcomes.
Once medically and neurologically stable, the overall function depends on attaining age-appropriate levels of independence and responsibility taking. The family, community, school, and rehabilitation teams are important in promoting physical, social, and emotional development in children with spina bifida.[Figure caption and citation for the preceding image starts]: Spine MRI scan showing tethered cordFrom the collection of Dr Nienke P. Dosa; used with permission [Citation ends].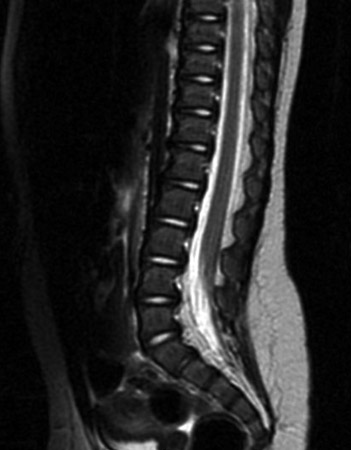
Adolescents and young adults
Many adolescents and young adults become socially isolated. Participation in peer activities is less than in the general population owing to a complex interplay of physical disability, incontinence, executive dysfunction, and non-verbal learning disability.[138][139] Anxiety and depression are common. Loss of ambulation can occur as youths gain weight and adult stature. When the structure of school and home routines is no longer in place, executive dysfunction can be unmasked. Studies have shown a decline in health and social participation beginning in late adolescence.[140] This is characterised by avoidable health complications such as pressure sores because skin checks are not done, difficulty in gaining or maintaining employment, and missed medical appointments because patients have difficulty with organisation and taking initiative due to executive dysfunction.
Pregnancy
Many women with spina bifida have normal pregnancies. However, there are few compiled data on outcomes and complications of pregnancy in this specific population.
Adults
Survival to adulthood has improved dramatically since the 1950s, although it is still less than for the general population. In 2 studies from the US, survival to adulthood ranged from 75% to 85%.[141][142] Survival to age 34 years was 94% among patients without shunts and 75% among those with shunted hydrocephalus. As survival has increased, the birth prevalence has decreased.[143] As a result, the majority of people with spina bifida in the US are now over 18 years of age.[144][145] With good preventative health measures and daily hygiene, long-term outlook may approach that of people without spina bifida. Close follow-up with specialists in neurosurgery, urology, and psychiatry is recommended throughout the patient's lifespan.[146] As the population is ageing since the advent of shunt surgery and bladder catheterisation, life expectancy is yet unknown. Generally speaking, patients with shunted hydrocephalus are at greater risk for early mortality.[147]
Use of this content is subject to our disclaimer