Case history
Case history
A 57-year-old man presents with persistent cough and shortness of breath. He was recently treated for pneumonia with a 10-day course of oral levofloxacin. He also complains of multiple painless nodular skin lesions on his arms and legs. He has no significant past medical history and prior to the illness was taking no medicines. He enjoys hunting and fishing as hobbies. He notes that his hunting dog also has similar skin lesions. Physical examination is significant for multiple 1.5 to 2 cm erythematous nodules, some with central ulceration, on the extremities. He also has consolidative lung findings on pulmonary auscultation. [Figure caption and citation for the preceding image starts]: Cutaneous blastomycosis on the forearmPersonal files of Larry Baddour, MD [Citation ends].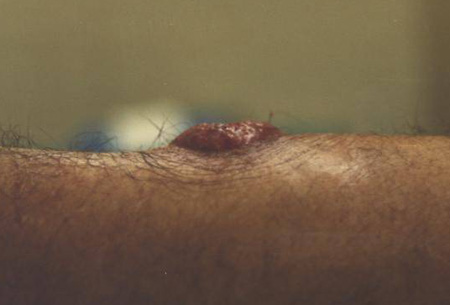
Other presentations
The majority of people acutely infected with Blastomyces dermatitidis develop asymptomatic, self-limiting pulmonary infections. The most common presentation is a mild-to-moderately severe community-acquired pneumonia that tends to involve the upper lobes. However, some patients can present with lung masses or progress to respiratory failure and adult respiratory distress syndrome.[4] Less common manifestations arise due to systemic spread of the infection. [Figure caption and citation for the preceding image starts]: Pulmonary blastomycosis with focal infiltrates on chest x-rayDr Robert Orenstein, DO, Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Scottsdale, AZ [Citation ends].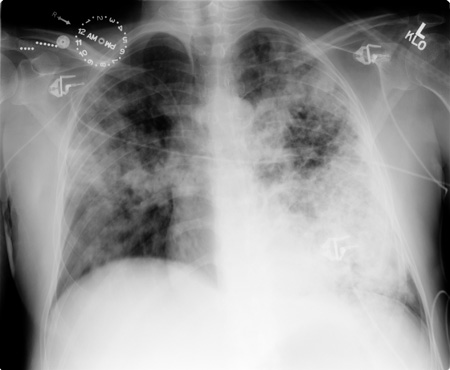 [Figure caption and citation for the preceding image starts]: Pulmonary blastomycosis presenting as a miliary pattern on chest x-rayDr Robert Orenstein, DO, Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Scottsdale, AZ [Citation ends].
[Figure caption and citation for the preceding image starts]: Pulmonary blastomycosis presenting as a miliary pattern on chest x-rayDr Robert Orenstein, DO, Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Scottsdale, AZ [Citation ends].
Cutaneous blastomycosis is the most common extrapulmonary presentation, and presents as painless nodules or non-healing ulcers mainly on the extremities. Cutaneous involvement usually results from disseminated disease.[4] Rarely, the skin is infected by direct inoculation via minor or major trauma. Primary osteoarticular involvement may result from haematogenous seeding, or secondary to direct bone invasion from overlying skin lesions, and patients can present with bone pain or septic arthritis. Central nervous system involvement can present either as acute or chronic aseptic meningitis or with space-occupying lesions on brain imaging with attendant neurological symptoms. Chronic prostatitis, which is always part of a disseminated process, is an unusual manifestation in men. Women can develop tubo-ovarian abscesses, endometritis, and salpingitis.[5][Figure caption and citation for the preceding image starts]: Cutaneous blastomycosis on the lower extremityLuAnn Ziemer, Office of Medical Photography, Mayo Clinic, Rochester, MN [Citation ends]. [Figure caption and citation for the preceding image starts]: Cutaneous blastomycosis on the lower extremityLuAnn Ziemer, Office of Medical Photography, Mayo Clinic, Rochester, MN [Citation ends].
[Figure caption and citation for the preceding image starts]: Cutaneous blastomycosis on the lower extremityLuAnn Ziemer, Office of Medical Photography, Mayo Clinic, Rochester, MN [Citation ends]. [Figure caption and citation for the preceding image starts]: Axial T1 gadolinium-enhanced MRI image of cerebral blastomycosisDr William Marshall, MD, Assistant Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester, MN [Citation ends].
[Figure caption and citation for the preceding image starts]: Axial T1 gadolinium-enhanced MRI image of cerebral blastomycosisDr William Marshall, MD, Assistant Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester, MN [Citation ends].
Use of this content is subject to our disclaimer