Investigations
1st investigations to order
lateral sacrococcygeal x-ray
Test
Suggests a coccygeal pain source.[19]
Different coccygeal configurations have been described:[4][19]
Type 1: normal, curved slightly forward, seen in 68% of the general population
Type 2: curved forward 90°
Type 3: sharply angulated at the first or second intercoccygeal joint
Type 4: anterior subluxation
Type 5: coccygeal retroversion with spicule
Type 6: scoliotic deformity.
Patients with coccygodynia are more likely to have type 3 and 4 configurations, and less likely to have type 1 configuration, than people without coccygodynia.[19][20][Figure caption and citation for the preceding image starts]: Lateral sacrococcygeal x-ray in a patient with post-traumatic chronic coccygodynia, showing sacrococcygeal synostosis (fusion, normal variant) and Co1-Co2 anterior subluxationFrom the personal collection of Dr R. Schrot [Citation ends].
Patients are more likely to have fusion of the sacrococcygeal joint (51% versus 37% in people without coccygodynia).[19][20]
Result
coccyx angulated >90°, sharply angulated, subluxed
dynamic lateral sacrococcygeal x-rays
Test
Used to compare changes between standing and painful sitting.
Radiographic instability, as evidenced by posterior subluxation and hypermobility (>20° of sacrococcygeal or intercoccygeal angulation), is seen in approximately 70% of patients.[16][21][Figure caption and citation for the preceding image starts]: Dynamic lateral sacrococcygeal x-ray in a patient with chronic idiopathic coccygodynia, showing 30° of anterior flexion while standingFrom the personal collection of Dr R. Schrot [Citation ends]. [Figure caption and citation for the preceding image starts]: Dynamic lateral sacrococcygeal x-ray in a patient with chronic idiopathic coccygodynia, showing 30° of anterior flexion while sittingFrom the personal collection of Dr R. Schrot [Citation ends].
[Figure caption and citation for the preceding image starts]: Dynamic lateral sacrococcygeal x-ray in a patient with chronic idiopathic coccygodynia, showing 30° of anterior flexion while sittingFrom the personal collection of Dr R. Schrot [Citation ends].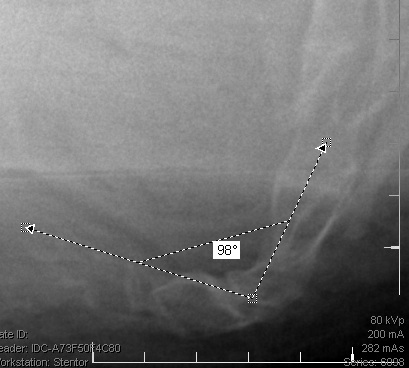
Other lesions include anterior subluxation and a bony spicule on the dorsal tip of the coccyx (seen in 5% and 14% of coccygodynia, respectively).[21]
Radiographic instability predicts excellent or good results after coccygectomy.[21]
Result
coccyx flexes >20° between standing and sitting, coccyx subluxes
Investigations to consider
MRI of the sacrum and coccyx
Test
Recommended to define normal and abnormal bony anatomy, and rule out less common causes of coccygodynia such as presacral tumours, perirectal abscess, or sacral intra-dural tumours.[20]
Masses should be further evaluated with gadolinium enhancement.
Result
may be normal, show degenerative changes at the sacrococcygeal or intercoccygeal articulations or, rarely, a sacral or pelvic mass
CT lumbosacral spine
Test
CT is used to define normal and abnormal bony anatomy and to evaluate sacrococcygeal trauma. Masses should be further evaluated with a CT scan. Lytic lesions may be present with infectious or neoplastic disease involving the coccyx.
Result
may be normal, or reveal fracture or subluxation of a sacro- or intercoccygeal segment, or lytic lesions
WBC count
Test
Ordered if pelvic infectious or inflammatory conditions are suspected, as evidenced by redness and swelling in the perineal area.
Result
normal or elevated in pelvic infection or inflammatory condition
erythrocyte sedimentation rate
Test
Ordered if pelvic infectious or inflammatory conditions are suspected, as evidenced by redness and swelling in the perineal area.
Result
normal or elevated in pelvic infection or inflammatory condition
Use of this content is subject to our disclaimer