Investigations
1st investigations to order
x-rays of neck, chest, abdomen
Test
Considered as the initial tests of choice to assess patients with suspected foreign body obstruction.
In young children, a mouth-to-anus radiograph should be obtained.
In older children and adults with suspected upper gastrointestinal foreign body, posteroanterior and lateral chest radiographs provide better localisation.
In oesophageal food impactions, a plain chest x-ray may be done to search for bony fragments that can lacerate the mucosa during extraction.
In adults with a suspected rectocolonic foreign body, a plain abdominal film radiograph, including an abdominal flat plate to identify the object and an upright film to evaluate for pneumoperitoneum, is useful.
Retained objects in the rectum can also ascend higher into the colon, as far as the hepatic flexure. If they perforate the colon, they may lodge in the retroperitoneal tissue, induce localised contained abscesses, lie free within the peritoneum, or even travel to distant sites in the body.[42][47]
Flat objects such as coins are usually seen in a coronal alignment on anteroposterior, or frontal, radiographs.[53] Metallic objects (except aluminium), most animal bones (except some fish bones, such as those of trout, mackerel, and herring), and glass materials are opaque on x-rays. Most plastic and wooden materials are not opaque on x-rays.[40][Figure caption and citation for the preceding image starts]: Plain abdominal radiology showing foreign body in the stomach lumenFrom the collection of Juan Carlos Munoz [Citation ends]. [Figure caption and citation for the preceding image starts]: Plain abdominal x-ray showing multiple foreign bodies. There were no signs of intestinal obstruction or perforationFrom: Canda AE. BMJ Case Reports. 2009;2009:bcr12.2008.1354 [Citation ends].
[Figure caption and citation for the preceding image starts]: Plain abdominal x-ray showing multiple foreign bodies. There were no signs of intestinal obstruction or perforationFrom: Canda AE. BMJ Case Reports. 2009;2009:bcr12.2008.1354 [Citation ends].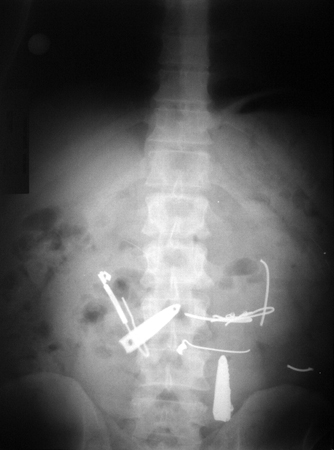
Result
metallic objects (except aluminium) and most animal bones (except some fish bones) are opaque; in perforation, posteroanterior and lateral x-rays of the neck and chest may show subcutaneous emphysema, pneumomediastinum, pneumothorax, or pleural effusion
FBC
Test
Should be part of the initial evaluation in any patient who presents with bleeding. Anaemia may range from mild to severe (rare cases) in patients with underlying medical conditions.
Result
normal in otherwise healthy patients; low haemoglobin should raise concern for possible bleeding
basic metabolic panel
Test
Should be part of the initial evaluation in patients who have been vomiting or bleeding.
Result
alterations in electrolytes can occur with vomiting, and an elevated urea/creatinine ratio can suggest upper gastrointestinal bleeding
prothrombin time (PT)/INR, PTT
Test
PT/INR and/or activated PTT should be tested in patients on anticoagulation or with suspected coagulopathy.
Causes of prolonged PT/INR include vitamin K deficiency, diet low in vitamin K (green and dark green vegetables, soybeans), chronic liver disease, alcohol misuse, oral contraceptive, use of anticoagulant drugs (warfarin).
Prolonged PTT may be the result of anticoagulation therapy, liver problems, lupus, and other diseases that result in poor clotting.
Result
typically normal
Investigations to consider
cardiac biomarkers and ECG
Test
Should be considered in patients presenting with atypical chest pain.
Result
should be normal; elevation in troponin may suggest cardiac ischaemia rather than a food bolus or foreign body ingestion as the cause of chest pain
CT of neck, chest, and/or abdomen
Test
A CT should be considered when multiple radiographs are inconclusive.
CT scans can be helpful in the detection of non-metallic foreign bodies and perforation.[47][51]
Non-metallic foreign bodies, especially fish bones and fragments of other objects (e.g., plastic objects), present a unique diagnostic problem due to their lack of opacity on radiographs and as such may require a CT scan.[40]
The European Society of Gastrointestinal Endoscopy clinical guideline recommends a CT scan in all patients with a suspected perforation or other complication that may require surgery.[34] Some paediatric guidelines suggest considering CT for radiolucent foreign bodies.[43]
Result
can reveal the location of both metallic and non-metallic foreign bodies, as well as perforation
MRI
laryngoscopy
Test
Can be used to evaluate for objects lodged at or above the cricopharyngeal area.
Result
FB at or above cricopharyngeal area
endoscopy
Test
Generally the first-line modality for the extraction of foreign bodies within the gastrointestinal tract (from esophagus to anus).[44][46][45]
[Figure caption and citation for the preceding image starts]: Endoscopic photograph of a food impaction in the lower oesophagus with evident concentric mucosal ring suggesting eosinophilic oesophagitisFrom the collection of Juan Carlos Munoz [Citation ends]. [Figure caption and citation for the preceding image starts]: Impacted food bolus removed from lower oesophagusFrom the collection of Juan Carlos Munoz [Citation ends].
[Figure caption and citation for the preceding image starts]: Impacted food bolus removed from lower oesophagusFrom the collection of Juan Carlos Munoz [Citation ends]. [Figure caption and citation for the preceding image starts]: Endoscope view showing foreign bodies in the stomach lumenFrom the collection of Juan Carlos Munoz [Citation ends].
[Figure caption and citation for the preceding image starts]: Endoscope view showing foreign bodies in the stomach lumenFrom the collection of Juan Carlos Munoz [Citation ends]. [Figure caption and citation for the preceding image starts]: Foreign bodies removed from the stomachFrom the collection of Juan Carlos Munoz [Citation ends].
[Figure caption and citation for the preceding image starts]: Foreign bodies removed from the stomachFrom the collection of Juan Carlos Munoz [Citation ends]. [Figure caption and citation for the preceding image starts]: (A) Endoscopic view of impacted nail-clipper in the duodenum. (B) Endoscopic removal of tie-clipFrom: Canda AE. BMJ Case Reports. 2009;2009:bcr12.2008.1354 [Citation ends].
[Figure caption and citation for the preceding image starts]: (A) Endoscopic view of impacted nail-clipper in the duodenum. (B) Endoscopic removal of tie-clipFrom: Canda AE. BMJ Case Reports. 2009;2009:bcr12.2008.1354 [Citation ends].
Result
can reveal and allow the extraction of a foreign body
Use of this content is subject to our disclaimer