Approach
Asymptomatic popliteal cysts require no treatment, but other diagnostic tests may be obtained to identify the underlying cause of the disease.
The treatment approach for a symptomatic patient depends on the severity of symptoms and response to conservative or percutaneous treatment.
Symptomatic: initial treatment
Patients with minor signs and symptoms such as fullness or mild discomfort in the popliteal fossa are managed conservatively. Treatments include physiotherapy and simple analgesics (e.g., aspirin or paracetamol), or non-steroidal anti-inflammatory drugs (NSAIDs).
Symptomatic: refractory to initial conservative treatment
For symptomatic patients with identified underlying intra-articular pathology, correction of the underlying pathology is the first line of treatment.
If a knee effusion is present, aspiration of the knee joint is usually beneficial. Simple analgesics (e.g., aspirin or paracetamol) may be used adjunctively for pain relief, or NSAIDs. Physiotherapy may also be indicated.
Popliteal cysts have been reported to rapidly improve following intra-articular injection of corticosteroids.[9] It is therefore acceptable to attempt corticosteroid injection in patients with significantly symptomatic popliteal cysts unresponsive to conservative treatments. Ultrasound-guided fenestration with injection has been described with reasonably good results.[23] Additional direct aspiration of the cyst may be performed in cases of larger fluid collections, although cysts may recur.[23]
Surgical treatment
Rarely performed and is only indicated in patients with extensive symptoms who fail conservative and percutaneous treatments.
It is the experience of some surgeons that simple excision of a popliteal cyst results in high incidence of recurrence. Surgical options have been described, including anterior open synovectomy, arthroscopic synovectomy, radiosynovectomy, capsulectomy, capsuloplasty with pedicle graft, and repair of joint capsule.
Arthroscopic resection facilitates management of the cyst (by arthroscopic decompression) and the associated intra-articular disorder. Surgery involves enlarging the interval between the semimembranosus and medial gastrocnemius, allowing the cyst contents to drain into the joint. Arthroscopic resection is effective, and is associated with reduced morbidity and recurrence compared with excision.[24][25][26][Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John Kelly IV; used with permission [Citation ends].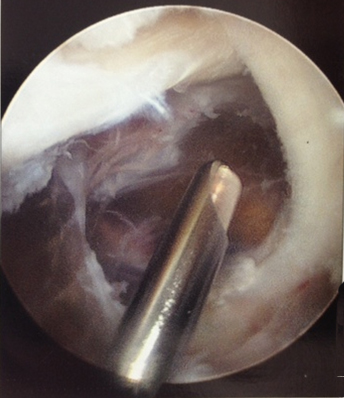 [Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Septae within a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].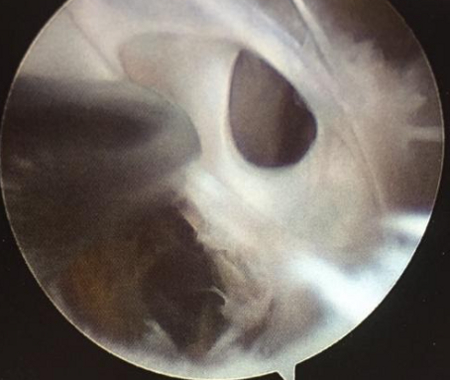
Use of this content is subject to our disclaimer