Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
injection with nonanesthetic agents
Injection modalities, including autologous blood, platelet-rich plasma, hyaluronic acid, and botulinum toxin, have been proposed as treatments for recalcitrant lateral and medial epicondylitis.
Autologous blood or platelet-rich plasma is injected into the tendons and is thought to stimulate a local inflammatory response. The use of injections with autologous blood/platelet-rich plasma may be considered as alternate treatments to surgical intervention, but the evidence for these therapies is currently limited.[94]
[ ![]() ]
The UK National Institute for Health and Care Excellence (NICE) recommends autologous blood products for the treatment of tendinopathy; however, their effectiveness is uncertain.[96]
]
The UK National Institute for Health and Care Excellence (NICE) recommends autologous blood products for the treatment of tendinopathy; however, their effectiveness is uncertain.[96]
Two systematic reviews in patients with lateral epicondylitis reported that autologous blood or platelet-rich plasma significantly improved pain and elbow function in the intermediate term (12-26 weeks), and that platelet-rich plasma injection improved function and pain at 24 weeks, compared with corticosteroid injections.[97][98]
However, a subsequent Cochrane review concluded that autologous blood/platelet-rich plasma injections provide little or no clinically important benefit for pain or function in patients with lateral elbow pain.[99] It also reported that it is uncertain whether the injections improve treatment success or pain relief (>50%).[99]
[ ![]() ]
]
Reduced pain following botulinum toxin injection has been reported in people with lateral epicondylitis, but there is also a high risk of complications, including digital paresis and weakness.[100][101][102][103]
Hyaluronic acid injections have been shown to improve pain and grip strength in patients with chronic lateral epicondylitis when compared with placebo. No serious adverse effects were reported and improvement persisted after 1 year.[104] However, few high-quality studies are available.
surgery
Surgical intervention for both medial and lateral epicondylitis is limited to refractory cases.[4][24][59][Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].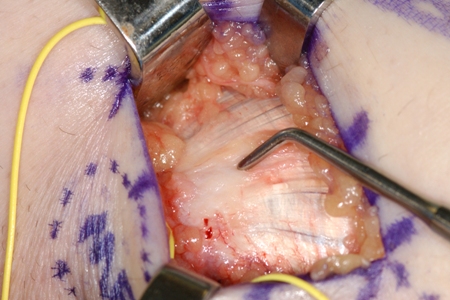 [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: pickups lifting off area of degenerative tendon after elliptical incision to excise this areaFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: pickups lifting off area of degenerative tendon after elliptical incision to excise this areaFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].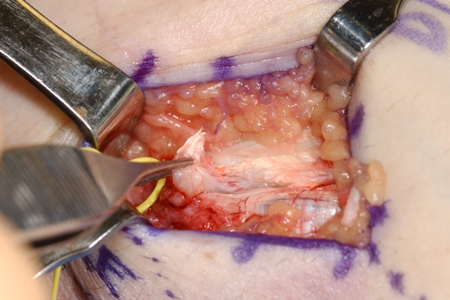 [Figure caption and citation for the preceding image starts]: Markings for swing incision location for patient with chronic refractory medial epicondylitisFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Markings for swing incision location for patient with chronic refractory medial epicondylitisFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].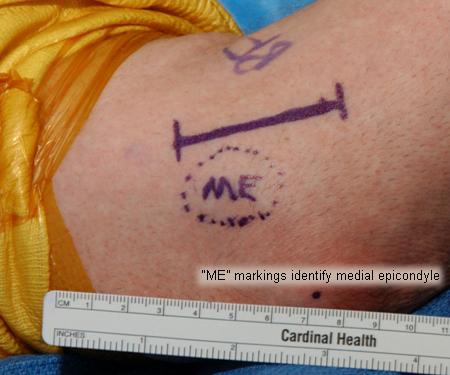 [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: degenerative tendon removedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: degenerative tendon removedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].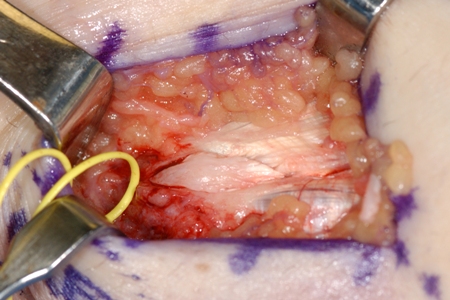 [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: medial epicondyle exposedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: medial epicondyle exposedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].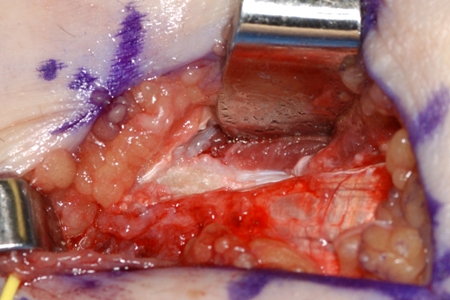
Surgical intervention for medial epicondylitis involves the open debridement and excision of the undersurface of the flexor pronator mass. Mean subjective estimate of elbow function has been found to improve from 38% to 98% of normal after surgery for medial epicondylitis.[86]
Possible adverse effects of surgery include injury to ulnar nerve and/or weakness with wrist flexion.
injection with nonanesthetic agents
Injection modalities, including autologous blood, platelet-rich plasma, hyaluronic acid, and botulinum toxin, have been proposed as treatments for recalcitrant lateral and medial epicondylitis.
Autologous blood or platelet-rich plasma injected into the tendons and is thought to stimulate a local inflammatory response. The use of injections with autologous blood/platelet-rich plasma may be considered as alternate treatments to surgical intervention, but the evidence for these therapies is currently limited.[94][95] The UK National Institute for Health and Care Excellence (NICE) recommends autologous blood products for the treatment of tendinopathy; however, their effectiveness is uncertain.[96]
Two systematic reviews in patients with lateral epicondylitis reported that autologous blood or platelet-rich plasma significantly improved pain and elbow function in the intermediate term (12-26 weeks), and that platelet-rich plasma injection improved function and pain at 24 weeks, compared with corticosteroid injections.[97][98]
However, a subsequent Cochrane review concluded that autologous blood/platelet-rich plasma injections provide little or no clinically important benefit for pain or function in patients with lateral elbow pain.[99] It also reported that it is uncertain whether the injections improve treatment success or pain relief (>50%).[99]
[ ![]() ]
]
Reduced pain following botulinum toxin injection has been reported in people with lateral epicondylitis, but there was also a high risk of complications, including digital paresis and weakness.[100][101][102][103]
Hyaluronic acid injections have been shown to improve pain and grip strength in patients with chronic lateral epicondylitis when compared with placebo. No serious adverse effects were reported and improvement persisted after 1 year.[104] However, few high-quality studies are available.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer