Approach
RVO frequently presents as sudden, painless, unilateral vision loss. Most affected patients are aged >65 years.[6] A patient with branch retinal vein occlusion (BRVO) can present with vision loss in 1 quadrant of their visual field, while a patient with central retinal vein occlusion (CRVO) presents with vision loss in the whole visual field. Similarly, a patient with a hemiretinal vein occlusion (HRVO) can present with a vision loss in the whole superior or inferior hemifield of vision, respecting the horizontal meridian.
History
Commonly, older patients have a history of hypertension, diabetes mellitus, atherosclerosis, cardiovascular disease, tobacco use, or glaucoma.[2][6][22] Younger affected patients are more likely to have a history of hypercoagulability or vasculitis.[17][18][19][23]
Commonly, patients with an RVO may present with symptoms of complications from BRVO, CRVO, or HRVO. Vision-threatening complications include macular edema and neovascularization. Patients with macular edema report decreased central vision. Those with a vitreous hemorrhage secondary to retinal neovascularization complain of floaters throughout their field of vision. A painful, red eye with vision loss could be a presentation of increased intraocular pressure in the setting of iris or angle neovascularization (commonly referred to as neovascular glaucoma).
Patients may have a history of ocular injections, retinal laser treatment, cataract surgery, or refractive surgery.[4][24]
Physical exam
Visual acuity is usually decreased, especially in patients with CRVO, macular edema, or vitreous hemorrhage. A visual acuity worse than 20/200 is a sign suggesting an ischemic CRVO.[9][10] A relative afferent pupillary defect would also suggest an ischemic CRVO.[9][10][25] Intraocular pressure should be checked in both eyes to assess the risk of glaucoma, which is a risk factor for RVO, and is elevated in an eye affected by neovascular glaucoma.[22] Confrontational visual field testing can help localize the retinal quadrant(s) affected by the RVO.
Perform slit lamp biomicroscopy with appropriate lenses to evaluate retinopathy (indirect ophthalmoscopy is preferable for examination of the far peripheral retina). During the slit lamp exam, check the iris for neovascularization and perform gonioscopy to rule out neovascularization of the angle.
Acutely, dilated fundus exam demonstrates venous tortuosity and dilation, intraretinal hemorrhages and thickening, and cotton-wool spots in the affected regions of the RVO. A BRVO would have these features in 1 quadrant and in the region of an arteriovenous crossing. An HRVO would have these features in either the superior or inferior retinal hemisphere. In a CRVO, all 4 quadrants of retinal tissue are affected. In addition, CRVO is more likely to feature optic nerve head edema.
Complications of RVO should be searched for during the dilated fundus exam. The presence or absence of macular thickening should be documented. Although more commonly found in CRVO and HRVO, neovascularization and/or vitreous hemorrhage may be found in any eye with RVO. Collateral vessel formation, either across the horizontal raphe in the macula (BRVO) or at the optic nerve head (CRVO), is a sign of chronicity.[Figure caption and citation for the preceding image starts]: Color photograph, right eye; central retinal vein occlusion; multiple intraretinal hemorrhages in each quadrantFrom the personal library of Dr Aziz Khanifar [Citation ends].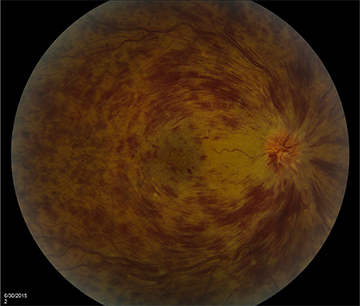 [Figure caption and citation for the preceding image starts]: Optical coherence tomogram, right eye; central retinal vein occlusion; large cystoid thickening throughout maculaFrom the personal library of Dr Aziz Khanifar [Citation ends].
[Figure caption and citation for the preceding image starts]: Optical coherence tomogram, right eye; central retinal vein occlusion; large cystoid thickening throughout maculaFrom the personal library of Dr Aziz Khanifar [Citation ends].
Tests
A fluorescein angiogram should be ordered whenever the diagnosis of RVO is suspected but not confirmed by clinical exam. In addition, fluorescein angiography provides information on complications of RVO that should be addressed when planning treatment. These complications include retinal ischemia, macular edema, and neovascularization. Presence of macular edema can be confirmed and quantified using optical coherence tomography (OCT). OCT may reveal intraretinal hyporeflectivity and thickening of the neurosensory retina (evidence of cystoid macular edema).[4] Subretinal hyporeflectivity (evidence of subretinal fluid) can be found in eyes with large amounts of macular edema. In BRVO, macular edema will be present asymmetrically; for example, for a superior BRVO, only the superior half of the macula will be edematous. OCT can also be used to evaluate response to therapy for macular edema. Electroretinography can also confirm the perfusion status of CRVO, especially in the setting of vitreous hemorrhage or significant intraretinal hemorrhage that prohibits utility of fluorescein angiogram, although it is rarely used in routine clinical practice.[25]
For younger patients with RVO, a thorough history should be taken, exploring the possibilities of either an altered coagulable state or a vasculitis as the underlying etiology. For young women, this includes determining whether the patient is using oral contraceptives. A limited diagnostic evaluation should then be completed, depending on the patient’s medical history. For altered coagulable states, this would include looking for activated protein C resistance, protein C deficiency, protein S deficiency, antithrombin III deficiency, elevated homocysteine, antiphospholipid antibody syndrome, and factor V Leiden. If appropriate, vasculitic diseases such as systemic lupus erythematosus (SLE) should be ruled out.
[Figure caption and citation for the preceding image starts]: Fluorescein angiogram, right eye; central retinal vein occlusion; delayed drainage of veins in each quadrantFrom the personal library of Dr Aziz Khanifar [Citation ends]. [Figure caption and citation for the preceding image starts]: Color photograph, left eye; branch retinal vein occlusion; multiple intraretinal images in quadrant of blocked veinFrom the personal library of Dr Aziz Khanifar [Citation ends].
[Figure caption and citation for the preceding image starts]: Color photograph, left eye; branch retinal vein occlusion; multiple intraretinal images in quadrant of blocked veinFrom the personal library of Dr Aziz Khanifar [Citation ends].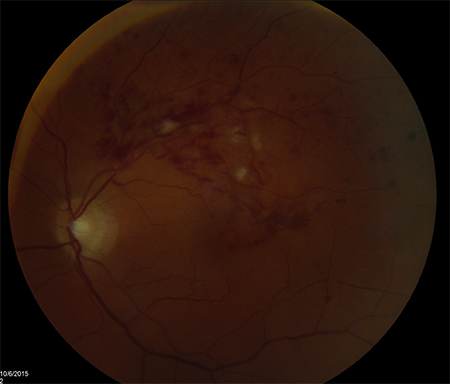 [Figure caption and citation for the preceding image starts]: Fluorescein angiogram, left eye; branch retinal vein occlusion; delayed drainage of blocked vein superotemporallyFrom the personal library of Dr Aziz Khanifar [Citation ends].
[Figure caption and citation for the preceding image starts]: Fluorescein angiogram, left eye; branch retinal vein occlusion; delayed drainage of blocked vein superotemporallyFrom the personal library of Dr Aziz Khanifar [Citation ends].
Use of this content is subject to our disclaimer