History and exam
Key diagnostic factors
common
edema
Patients may present acutely with overt nephrotic syndrome with edema. [Figure caption and citation for the preceding image starts]: Facial edema in a child with nephrotic syndromeFrom the collection of Dr M. Dixit, Medical Director, Florida Children's Kidney Centre; Dr R. Mathias, Chief, Pediatric Nephrology, Nemours Children's Clinic, Orlando, FL [Citation ends].
More commonly seen in primary FSGS.
foamy urine
Due to high levels of protein in the urine.
hypertension
Can occur due to increased salt retention and volume overload, or renal dysfunction with decreased glomerular filtration rate.
uncommon
Muehrcke lines
White banding on the nails due to hypoalbuminemia. [Figure caption and citation for the preceding image starts]: Muehrcke lines in a patient with hypoalbuminemia due to nephrotic syndromeFrom Muehrcke RC. The finger-nails in chronic hypoalbuminaemia: a new physical sign. Br Med J. 1956 Jun 9;1(4979):1327-8 [Citation ends].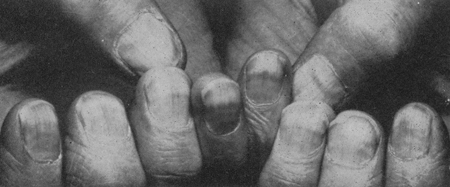
xanthelasma and xanthomata
Cholesterol deposits in the skin due to hypercholesterolemia. [Figure caption and citation for the preceding image starts]: Xanthomata in a patient with severe hyperlipidemiaFrom Watkins PJ. Cardiovascular disease, hypertension, and lipids. BMJ. 2003 Apr 19;326(7394):874-6 [Citation ends].
Other diagnostic factors
common
uncommon
lymphadenopathy
Generalized lymphadenopathy in HIV patients.
Peripheral lymphadenopathy in patients with systemic lupus erythematosus, which causes non-FSGS nephrotic syndrome.
skin rash
HIV-positive patients may have rashes or postinfective scars, especially shingles.
A photosensitive skin rash may indicate systemic lupus erythematosus, which causes non-FSGS nephrotic syndrome.
oral lesions
Ulcers, angular cheilitis, thrush, oral hairy leukoplakia, oral Kaposi sarcoma in HIV-positive patients.
nephrectomy scar
A solitary or transplanted kidney is at increased risk of secondary FSGS.
Risk factors
strong
male sex
Males have 1.5- to 2-fold greater risk than females of developing FSGS-induced end-stage renal failure.[8]
black race
A 4- to 7-fold greater risk than white or Asian people of developing FSGS-induced end-stage renal failure.[8][9] This may be partly explained by mutations in nonmuscle myosin heavy chain 9 (MYH9), which are associated with primary and HIV-induced FSGS and are more common in black patients.[9] Apolipoprotein L1 (APOL1) gene polymorphisms are also associated with FSGS in black patients and appear to be expressed almost exclusively in individuals of African descent.[18][19]
family history of FSGS
Some forms of FSGS are inherited and a positive family history may suggest a genetic cause.
The majority of genetic causes of FSGS in children follow an autosomal recessive pattern with mutations in the genes nephrin (NPHS1), podocin (NPHS2), and phospholipase C epsilon 1( PLCE1) being the most common.[16] Autosomal dominant causes of FSGS are more common in adolescents and adults. Major genes implicated in autosomal dominant FSGS include alpha-actinin 4 (ACTN4), inverted formin 2 (INF2), and the transient receptor potential cation 6 channel (TRPC6).[15] MYO1E mutations have been associated with childhood-onset, glucocorticoid-resistant FSGS.[17]
heroin abuse
Presumed mechanism is a direct toxic effect on the podocyte.
use of known causative medications
Interferon alfa, lithium, sirolimus, and pamidronate.[4] The presumed mechanism is a direct toxic effect on the podocyte.
chronic viral infection
HIV is the most common cause. Rarer causes include persistent parvovirus B19 infection, cytomegalovirus, hepatitis B and C, and SARS-CoV-2.[4]
weak
solitary kidney
Usually due to nephrectomy or congenital.
Produces compensatory glomerular hyperfiltration in the remaining kidney, which predisposes to FSGS.
pre-existing renal disease
Reflux nephropathy and renal dysplasia may cause secondary FSGS.
kidney transplant
Chronic allograft nephropathy can cause secondary FSGS.
acute renal ischemia
Renal thromboembolism is a rare cause of secondary FSGS.
Use of this content is subject to our disclaimer