Urgent considerations
See Differentials for more details
Hoarseness may indicate a serious underlying pathology. Acute onset of hoarseness with breathing difficulties or prolonged hoarseness, in both adults and children, requires urgent evaluation to rule out a laryngeal malignancy, airway obstruction, recurrent respiratory papilloma, or vocal fold paralysis.
Chronic hoarseness may be a sign of vocal fold paralysis due to a mediastinal mass or lung tumor.[37][38]
Treatment for patients with acute or chronic voice problems should not be initiated until the above diagnoses of concern have been ruled out.
Airway obstruction
Some of the conditions that cause hoarseness can result in airway obstruction if left untreated. They include:
Vocal fold cancer and other laryngeal malignancies [Figure caption and citation for the preceding image starts]: Vocal fold cancerFrom the collection of the University of Wisconsin School of Medicine and Public Health [Citation ends].

Reinke edema [Figure caption and citation for the preceding image starts]: Reinke edemaFrom the collection of the University of Wisconsin School of Medicine and Public Health [Citation ends].

Recurrent respiratory papilloma. [Figure caption and citation for the preceding image starts]: Recurrent respiratory papillomaFrom the collection of the University of Wisconsin School of Medicine and Public Health [Citation ends].

Undiagnosed, recurrent respiratory papilloma can result in airway obstruction needing tracheostomy and can be fatal if there is uncontrolled spread in the airway.[39][40]
Patients present with gradual or acute onset of inspiratory or biphasic stridor, noisy resting breathing, dyspnea, respiratory distress with accessory muscle use and tachypnea, shortness of breath while speaking with the inability to complete sentences in a single breath, a nonproductive cough, and/or the sensation of a blockage in the neck. Symptoms may initially be present only during exercise, but eventually occur with reduced amounts of exertion and are worse when the patient is in a supine position.
Immediate treatment depends on the underlying cause of airway obstruction. Treatment in adults should be initiated following a flexible fiberoptic transnasal exam of the airway. Medical management may assist in improving symptoms and lengthen the amount of time available for preparing a surgical procedure such as tracheostomy. Orotracheal intubation, whenever possible, is the preferred method of securing the airway, but local factors such as bleeding from a laryngeal tumor, and patient factors such as obesity, lack of neck extension, or comorbidity may reduce the safety of this procedure. A rigid bronchoscope may be used to bypass firm obstructing tumors, allowing a tracheostomy to be performed. Tracheostomy should be performed with the patient spontaneously ventilating. Therefore, heavy sedation and paralytics should be avoided.
Malignant/premalignant conditions
Vocal fold cancer [Figure caption and citation for the preceding image starts]: Vocal fold cancerFrom the collection of the University of Wisconsin School of Medicine and Public Health [Citation ends].
Hoarseness in a person who smokes or has a history of tobacco use should be urgently investigated, as it is frequently an early - and often the sole - symptom of vocal fold cancer. If detected early, laryngeal malignancies can be effectively treated; 5-year survival rates are around 62% to 64%.[41][42] The priority of treatment is preservation of laryngeal structure and tissue to maintain the airway and conserve normal voice production and swallowing.
If left untreated, laryngeal cancer can spread locally within the larynx, potentially causing airway obstruction, and to regional cervical lymph nodes, allowing risk of distant metastasis.[9]
Tumors of the larynx are the most common cause of misdiagnosis of unilateral vocal fold paralysis.[43]
Tumors of the neck, mediastinum, and lung
Lead to unilateral vocal fold paralysis if they are along the course of the recurrent laryngeal nerve. They require urgent evaluation and treatment.
Leukoplakia [Figure caption and citation for the preceding image starts]: LeukoplakiaFrom the collection of the University of Wisconsin School of Medicine and Public Health [Citation ends].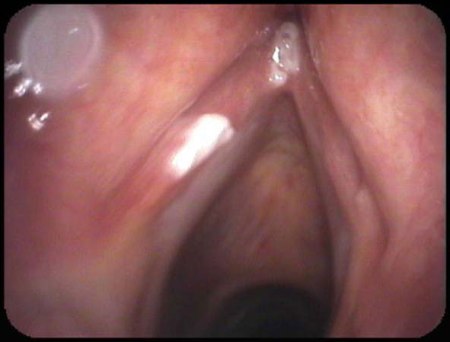
A premalignant change of vocal cord epithelium requiring early recognition and intervention to avoid progression to a malignant lesion.[34]
Infants and children
Voice changes with or without noisy breathing in infants and children require early assessment and laryngeal visualization to rule out recurrent respiratory papilloma (more severe with young onset) and vocal fold paralysis.
Airway distress and obstruction in the pediatric population should be evaluated and managed in the operating room.
Use of this content is subject to our disclaimer