Tests
1st tests to order
12-lead ECG
Test
Sinus bradycardia: regular P-wave followed by QRS at a rate of <50 bpm. Ambulatory ECG monitoring is helpful to correlate symptoms with heart rate.[41]
Sinus nodal pauses or arrest: long RR cycle length, which is longer than the RR interval of the underlying sinus rhythm. [Figure caption and citation for the preceding image starts]: ECG showing sinus pauseFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].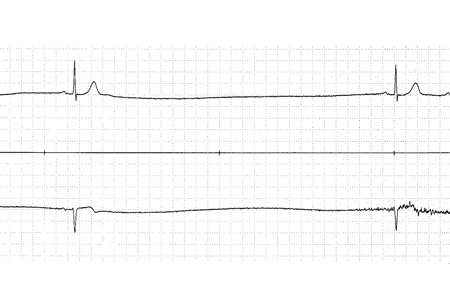
Sinus nodal exit block: an absent P-wave and prolongation of the RR cycle length, usually twice the underlying sinus RR interval.
Tachy-brady syndrome: episodic periods of tachycardia (usually atrial flutter, atrial fibrillation, or atrial tachycardia), followed by termination of the tachycardia leading to sinus arrest or long sinus pauses, followed by sinus bradycardia.[Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].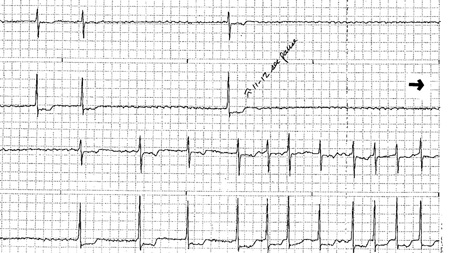 [Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing tachy-brady syndromeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].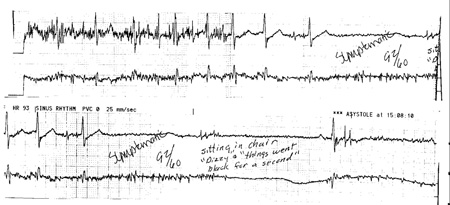
First-degree atrioventricular (AV) block: fixed prolongation of the PR interval of >0.2 seconds.[13][Figure caption and citation for the preceding image starts]: ECG showing first-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].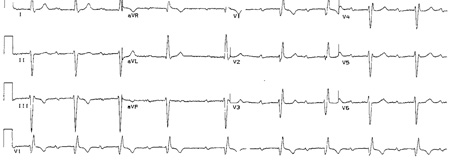
Mobitz I AV block: grouped beating with a constant PP interval, lengthening in the PR interval, and changing (usually shortening) RR intervals with the cycle ending with a P-wave not followed by a QRS complex. As the PR interval gradually prolongs, the RR interval tends to stay the same or shortens.[14][Figure caption and citation for the preceding image starts]: ECG showing Mobitz I (Wenckebach) second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].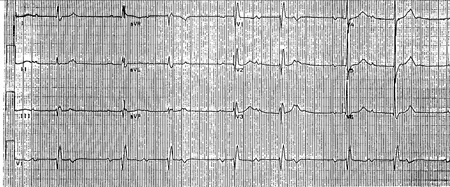 [Figure caption and citation for the preceding image starts]: ECG showing Mobitz I (Wenckebach) second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing Mobitz I (Wenckebach) second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].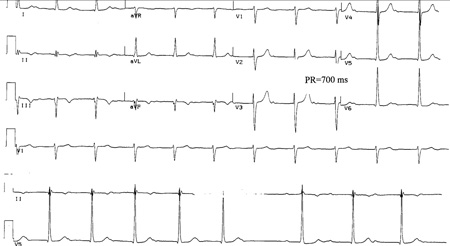 [Figure caption and citation for the preceding image starts]: ECG showing Mobitz I (Wenckebach) second-degree atrioventricular (AV) block during acute inferior wall myocardial infarctionFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing Mobitz I (Wenckebach) second-degree atrioventricular (AV) block during acute inferior wall myocardial infarctionFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
Mobitz II AV block: associated with single nonconducted P-waves with a constant PP interval and constant PR intervals (no change in the PR of >0.025 seconds).[15][Figure caption and citation for the preceding image starts]: ECG showing Mobitz II second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].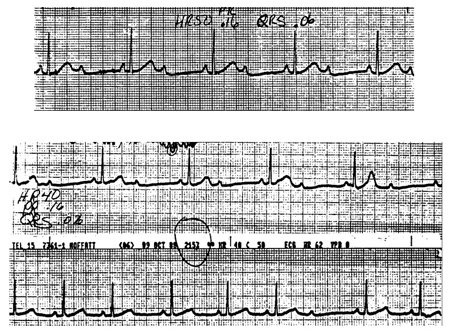 [Figure caption and citation for the preceding image starts]: ECG showing Mobitz II second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing Mobitz II second-degree atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
2:1 AV block: only one PR interval to examine before the blocked P-wave and 2 P-waves for every QRS complex. Block can be at the level of the AV node or the His-Purkinje system. If the QRS is narrow, the level of the block is probably in the AV node (which is more benign). If the QRS is wide (owing to bundle-branch block or other conduction delay), block in the AV node is still most common but block in the His-Purkinje system is more frequent than when the QRS complex is narrow.[Figure caption and citation for the preceding image starts]: ECG showing 2:1 atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: ECG showing 2:1 atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing 2:1 atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].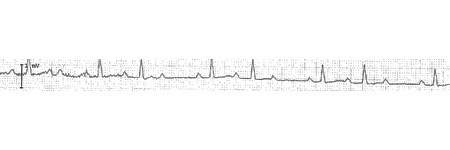
High-degree: more than one sequentially blocked P-wave. Block can be at the level of the AV node or the His-Purkinje system as is the case with 2:1 AV block.
Third-degree AV block: occurs when there are no conducted impulses from the atria to the ventricles. There is no consistent PR relationship. May occur with ventricular or junctional escape rhythm.[Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].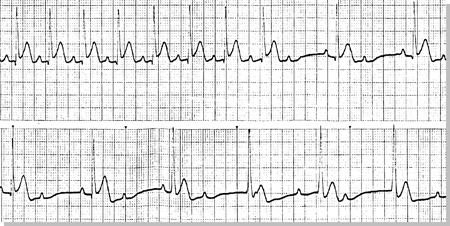 [Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) blockFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with ventricular escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with ventricular escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].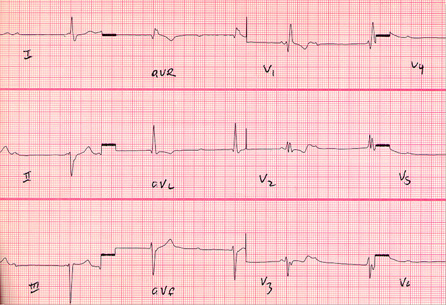 [Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with ventricular escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with ventricular escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].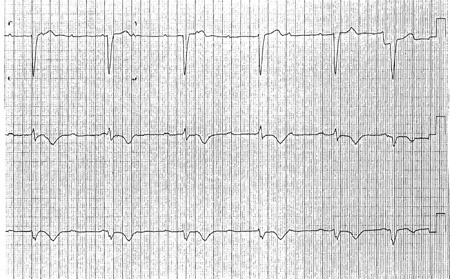 [Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with junctional escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing complete atrioventricular (AV) block with junctional escapeFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
Paroxysmal AV block: normal AV nodal conduction followed by sudden block of AV conduction associated with a long pause and multiple blocked P-waves, with subsequent resumption of AV conduction. This may begin with an ectopic impulse.
Vagotonic AV block: slowing of the sinus node with prolongation of the PR interval followed by AV block owing to transient abrupt increase in parasympathetic tone.
Congenital complete heart block: usually associated with a narrow QRS complex escape rhythm arising in the AV node.
Escape rhythms may also occur in AV block, such as atrial (abnormal P-wave and decreased PR interval), junctional (above the bundle of His, produces a rate of approximately 40-60 bpm and narrow QRS complexes), and ventricular rhythms (below the bundle of His, produces a slower rate of 20-40 bpm and wide QRS complexes).[Figure caption and citation for the preceding image starts]: ECG showing junctional rhythmFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
Isorhythmic dissociation: when the atrial rate is the same (or nearly the same) as the ventricular rate but the P-wave is not conducted.
Interference dissociation: when P-waves and QRS rates are similar but, occasionally, the atria conduct to the ventricles. [Figure caption and citation for the preceding image starts]: ECG showing interference atrioventricular (AV) dissociationFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: ECG showing interference atrioventricular (AV) dissociationFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: ECG showing interference atrioventricular (AV) dissociationFrom the collection of Brian Olshansky, MD, FAHA, FACC, FHRS, FESC; used with permission [Citation ends].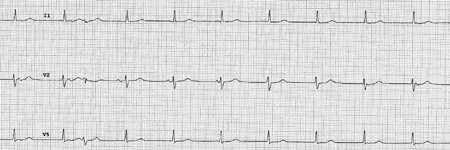
Result
may show sinus bradycardia with or without sinus arrhythmia, AV block with junctional or ventricular escape, His-Purkinje system disease, bradycardia, and AV block in a setting of myocardial infarction; deep T-wave inversions across the precordium indicative of a neurologic event may occur in conjunction with sinus bradycardia
Holter monitoring
Test
Enables correlation of symptoms with episodes of bradycardia. Diagnostic clues obtained in 50% to 70% of patients.[42][43] However, specificity is low.
Events can be missed if symptoms do not occur in the 24- to 48-hour monitoring period.
Asymptomatic bradycardia and pauses (especially nocturnal) are not uncommon in the normal heart and are probably nondiagnostic.
First-degree atrioventricular (AV) block or Mobitz type I AV block may be noted while patients are asleep owing to high vagal tone.
May help distinguish the location of the block (i.e., AV node versus His-Purkinje system) in 2:1 and high-degree AV block.
Result
sinus pauses; sinus arrest; second- or third-degree AV block; severe sinus bradycardia with symptoms
event monitor/mobile cardiac telemetry
Test
Used widely and can be worn for up to 30 days.
Earlier designs were patient triggered; however, newer-generation monitors have autotriggering capabilities and implantable-loop recorders.
Smartphone event monitors convert cardiac electric signal to an ultrasound FM sound signal, which is then demodulated to a digital ECG tracing. The ECG is generated in real time and can also be stored and instantaneously transmitted to a secure server for further analysis. Photoplethysmographic-based smart devices (e.g., watches) may also be used.
May be used if severe sinus node dysfunction (e.g., sinus exit block, sinus pauses, sinus arrest, or tachy-brady syndrome) is suspected but cannot be documented.
Particularly useful in diagnosing Mobitz I atrioventricular (AV) block.
Result
sinus pauses; sinus arrest; second- or third-degree AV block; severe sinus bradycardia with symptoms
exercise testing
Test
Subnormal increase in heart rate after exercise (chronotropic incompetence) can be useful in diagnosing sinus node dysfunction.[41][42][44]
However, sensitivity and specificity are unclear and results obtained may not be reproducible.[45]
Even so, exercise-induced atrioventricular (AV) block, even if asymptomatic, can be significant and suggests disease of the His-Purkinje system.
Identifying symptoms due to sinus bradycardia can be difficult; however, exercise testing can be useful to help determine sinus node dysfunction as the cause of symptoms.
Useful in determining level of block in Mobitz I.
Result
exercise-induced AV block; chronotropic incompetence
carotid sinus massage
Test
Used in the evaluation of carotid sinus hypersensitivity, which causes symptomatic bradycardia and is associated with sinus node dysfunction.[41]
Diagnostic yield can be increased by performing this during head-up tilting.[46]
Performed under continuous ECG monitoring.
Each carotid artery should be palpated and auscultated for a bruit.
Neck is extended and turned away from the examiner and pressure is applied with a circular movement over each carotid artery (one at a time) at the point where the carotid artery meets the angle of the jaw, the approximate location of the carotid sinus.
Massage is performed for 5-10 seconds in both supine and erect positions.
Contraindications include presence of a carotid bruit, a prior stroke, or transient ischemic attack unless imaging has shown no significant carotid disease, a myocardial infarction within the past 6 months, and a history of ventricular arrhythmias.
Can help diagnose Mobitz I and II atrioventricular (AV) block; it will accentuate Wenckebach in the AV node but will have an opposite effect if the block is below the His bundle.
May help distinguish the location of the block (i.e., AV node versus His-Purkinje system) in 2:1 and high-degree AV block. It may improve block in the His-Purkinje system by slowing the sinus and AV nodal inputs to the His-Purkinje system, enabling the His-Purkinje system a longer period to recover between inputs.
Result
pause of >3 seconds with symptoms suggests cardioinhibitory response indicative of carotid sinus hypersensitivity
echocardiogram
Test
Although it provides no direct diagnostic role, it provides valuable information regarding underlying heart disease that can influence management decision making.[41]
For example, if a patient is scheduled for pacemaker placement for complete heart block, a finding of a left ventricular ejection fraction of <30% may indicate that an implantable cardioverter defibrillator is needed in addition to a pacemaker.
Result
underlying structural heart disease, such as ventricular dysfunction or valvular heart disease
thyroid function tests
Test
Indicates decreased production of thyroid hormone (thyroxine) from the thyroid gland.[41]
All metabolically active cells in the body, including the heart, require thyroid hormone.
Bradycardia is due to alterations in metabolic processes or myxedematous changes.
Result
elevated thyroid-stimulating hormone in hypothyroidism
basic metabolic panel
Test
Potassium and calcium are essential for cardiac action potential and intrinsic pacemaker function.[41]
Derangements provide important clues as to the etiology of bradycardia.
Result
hypokalemia or hyperkalemia; hypocalcemia or hypercalcemia
arterial blood gas
Test
Acidosis can be a cause of bradycardia.
Result
acidemia
cardiac biomarkers
Test
Cardiac enzymes should be obtained if bradycardia is associated with ECG changes suggestive of myocardial infarction.
Creatine kinase (CK) is not specific for myocardial damage and can be released with any muscle damage. The isoenzyme CK-MB is more cardiac-specific but can also be released from skeletal muscle.
Troponins are highly specific for myocardial damage.
Result
elevation of CK, CK-MB, and troponin in myocardial infarction
serum digoxin level
Test
Patients who have junctional bradycardia and who are prescribed digoxin should have a serum digoxin level checked.
Result
depends on dose and drug-metabolism factors; may be in toxic range
serum creatinine
Test
Patients with chronic bradycardia may have evidence for worsening renal function.
Result
elevated if impaired renal function
Tests to consider
implantable-loop recorder
Test
Subcutaneous monitoring device used for the detection of cardiac arrhythmias.
Typically implanted under local anesthesia in the left parasternal or pectoral region. Small devices can be inserted by a qualified physician using an injection approach, and can be used for monitoring for up to 3 years.
Useful modality if a patient has intermittent symptoms suspected to be secondary to a bradyarrhythmia but with no ECG abnormalities and negative Holter and/or event monitoring. Safe and efficacious in these settings.[47][48]
Stores recorded ECG strips either when the device is activated by the patient or when activated automatically according to programmed threshold criteria. Periodic interrogation of the device can retrieve this information.
Also useful to rule out bradyarrhythmia as a cause of the patient's symptoms by identifying normal sinus rhythm at the time of a symptom event of interest.
Reduce/prevent recurrent symptoms.[47]
May be used if severe sinus node dysfunction (e.g., sinus exit block, sinus pauses, sinus arrest, or tachy-brady syndrome) is suspected but cannot be documented.
Particularly useful in diagnosing Mobitz I atrioventricular (AV) block.
Result
sinus pauses; sinus arrest; second or third-degree AV block; severe sinus bradycardia with symptoms
tilt-table testing
Test
Used to evaluate the adequacy of the autonomic system, especially when there is suspicion of neurocardiogenic syncope. Commonly used method is head-upright tilting, which causes dependent venous pooling and thereby provokes the autonomic response.[41]
Result
classic neurocardiogenic response is a sudden drop in blood pressure followed by bradycardia, reflecting a high vagal tone
Lyme titers
Test
Particularly if history of travel to endemic areas. Lyme disease most commonly presents as atrioventricular nodal conduction delay.[41]
Result
elevated IgG and IgM titers
electrophysiology testing
Test
Recommended when symptoms cannot be correlated clearly and when significant bradyarrhythmias are suspected but cannot be diagnosed by noninvasive modalities.[41]
Testing can be useful in patients with atrioventricular (AV) block and no clear symptom association, patients with symptoms of bradycardia and in whom AV block is suspected but not documented, and when the site of AV block cannot be determined reliably by surface tracings.
His-ventricle interval of >100 milliseconds in a patient with bradycardia, even in the absence of symptoms, is a high-risk finding.[49][50]
Overall, the role of electrophysiologic testing for bradycardia is limited, owing to low sensitivity and specificity. Positive findings may not be the reason for symptoms.[51][52]
May be used if severe sinus node dysfunction (e.g., sinus exit block, sinus pauses, sinus arrest, or tachy-brady syndrome) is suspected but cannot be documented.
Atrial pacing progressively shorter cycle lengths during an electrophysiology study can manifest Mobitz type I in subjects with normal or abnormal AV node conduction.
Useful to demonstrate the location of the block (i.e., AV node versus His-Purkinje system) in 2:1 and high-degree AV block.
Result
shows quantitative measurement of sinus node, AV node, and His-Purkinje system dysfunction
nocturnal pulse oximetry or overnight polysomnography
Test
Useful for patients with symptoms suspicious for obstructive or central sleep apnea, including daytime somnolence, multiple night-time awakenings, morning headaches, loud snoring, dry mouth on awakening.
Result
sinus bradycardia; sinus pauses or sinus arrest; also tachyarrhythmias such as atrial fibrillation
Use of this content is subject to our disclaimer