Case history
Case history #1
A 5-year-old white boy is brought in to the orthopedic clinic by his mother with complaints of a limp favoring the right side with no associated pain. This painless limp had started insidiously 3 weeks earlier and was first noticed by the school physical education teacher. The mother notes that it has recently been getting worse. He is one of three siblings and lives with his single mother. The other siblings include an elder sister (from his mother's earlier marriage) and a younger brother. His mother's current partner is a heavy smoker. His mother recalls that a year earlier he came from school and complained of right knee pain. This was initially overlooked for a few days, but when it persisted he was taken to the primary care physician who reassured his mother but did not arrange follow-up. The symptoms had recurred the following month when he was taken to the ER and blood tests and x-rays were reportedly normal.
Case history #2
A 7-year-old girl presents with a painless limp, although she has been treated for acute pain in the past. She has a free range of hip motion. Plain anteroposterior and frog lateral radiographs reveal Legg-Calvé-Perthes disease of the right hip. She undergoes screening of the right hip under a general anesthetic with an arthrogram to determine the best position of right femoral head containment in the hip joint. A surgical containment is performed by way of a varus lateral opening wedge osteotomy of the proximal femur, fixed with an AO (Arbeitsgemeinschaft fur Osteosynthesefragen) 3.5 mm precontoured plate and held with 3.5 mm AO screws, is performed. She is kept non-weight-bearing post-procedure. A radiograph 4 weeks later reveals a good containment of the hip joint, satisfactory alignment at the osteotomy and some early callus formation medially. A further radiograph 3 months postoperatively shows a good union at the osteotomy and a well-contained hip joint. Weight-bearing and resumption of normal activities is then allowed progressively. [Figure caption and citation for the preceding image starts]: AP radiograph of a patient with Perthes diseaseFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends]. [Figure caption and citation for the preceding image starts]: Frog lateral radiograph of a patient with Perthes diseaseFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].
[Figure caption and citation for the preceding image starts]: Frog lateral radiograph of a patient with Perthes diseaseFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends]. [Figure caption and citation for the preceding image starts]: Surgical containmentFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgical containmentFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends]. [Figure caption and citation for the preceding image starts]: Postoperative radiograph at 4 weeksFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].
[Figure caption and citation for the preceding image starts]: Postoperative radiograph at 4 weeksFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].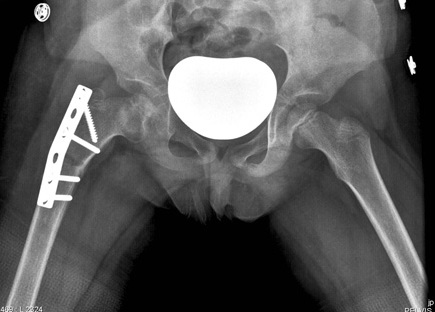 [Figure caption and citation for the preceding image starts]: Postoperative radiograph at 3 monthsFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].
[Figure caption and citation for the preceding image starts]: Postoperative radiograph at 3 monthsFrom the personal collection of Jwalant S. Mehta, MS (Orth), MCh (Orth), FRCS, FRCS (Orth) [Citation ends].
Other presentations
The typical age of presentation varies between 4 and 8 years but can range from 2 to 12 years, with several reports of involvement in adolescents. The usual phenotype of a child with Legg-Calvé-Perthes (Perthes) disease is short stature, delayed bone age, and hyperactivity. A limp is the most common presentation with a large proportion being unilateral afflictions. Bilateral involvement is seen in up to 10% to 12% of the cases; however, both hips are rarely at the same stage of the disease at any given time. Pain may vary in site, intensity, and radiation patterns. It may be referred to the knee, thigh, groin, or buttocks. Perthes disease is a nontraumatic condition, although a history of minor trauma may be noted.
Use of this content is subject to our disclaimer