Etiology
The true etiology of idiopathic clubfoot is unknown.[10][11] It is probably influenced by both environmental and genetic factors, resulting in a multifactorial etiology.[12]
Theories include arrest of normal development in the early fetus; a fibrotic response similar to Dupuytren contracture; a germ plasm defect in cartilage anlage; neuromyogenic imbalance of the peroneal muscles; or an in-utero compartment syndrome. Environmental influences have also been suggested: one Scottish study found a predominance in babies born in March and April, although a US study did not find similar results.[10][11] Clubfoot may also result from various syndromes such as Freeman-Sheldon or Mobius, as well as neuromuscular-type conditions such as arthrogryposis and spina bifida. Teratogenic agents such as sodium aminopterin and d-tubocurarine have been shown to cause clubfoot deformities.[8]
Pathophysiology
Ligaments that have been biopsied in infants with clubfeet show collagen fibers that are densely packed with a wavy appearance.[13][14][15][16] The ligaments of the posterior and medial tarsal and ankle joints are thickened, resulting in the hindfoot in varus, adduction, and equinus positions. The talus is plantar flexed with some medial rotation, resulting in the navicular being medially displaced. The tendons of the tibialis anterior, extensor hallucis, and extensor digitorum are medially displaced. The sum of the deformities results in the forefoot being pronated relative to the hindfoot supination. [Figure caption and citation for the preceding image starts]: Three-dimensional view of clubfoot deformity in an adolescent, showing the classic equinus, varus, and adduction deformitiesFrom the collection of Scott E. Van Valin [Citation ends].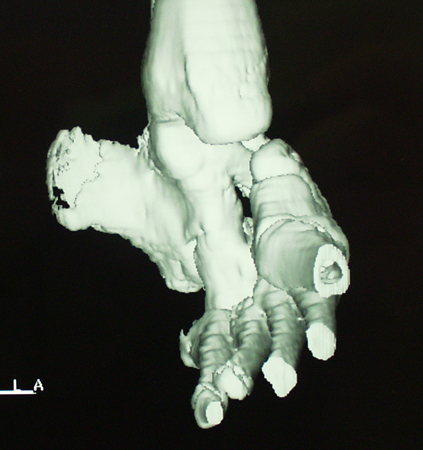
Classification
Idiopathic clubfoot[5]
The deformity is not correctable on exam. Rigid with noted atrophy. May be generalized to moderate or severe.
Postural clubfoot[5]
Not a true clubfoot. The deformity is fully correctable on exam. Rigidity and atrophy are not present. An in-utero postural deformity.
Nonidiopathic (syndromic) or teratologic type[5]
Extremely severe clubfoot deformity. Difficult to treat, with a higher nonoperative failure rate. May result from neuromuscular disease. Various neuromuscular-type diseases are associated with clubfoot, including arthrogryposis, cerebral palsy, diastrophic dysplasia, polio, spina bifida, and syndromes such as amniotic band, Down, Freeman-Sheldon, or Mobius.
Use of this content is subject to our disclaimer