Etiology
Excessive friction of the distal iliotibial band (ITB) sliding over the lateral femoral epicondyle occurs as the knee flexes during deceleration into stance-phase running.[5] This is termed the impingement zone at approximately 30° of knee flexion. Cycling has pedal-reaction forces that are significantly lower than running but the distal iliotibial band has similar stress at the impingement zone during flexion and extension. Intrinsic risk factors or training factors can cause excessive friction, and patients typically will have a combination of each. Runners predisposed to this injury are typically in a phase of overtraining and often have underlying weakness of the hip abductor muscle.[15][17][18] The runner may describe a rapid progression in weekly mileage.[15]
Intrinsic factors that contribute to ITB tightness and muscle weakness (quadriceps and gluteus medius) include: genu varum (bow leg); pes cavus (high arch); prominent lateral femoral epicondyle; tight iliotibial tract, lateral retinaculum, tensor fascia lata, rectus femoris, and hamstrings.[19][20] Proximal ITB syndrome is a condition that involves stress to the iliotibial band origin at the iliac crest.[8] This is a condition reported uniquely in women runners, influenced by increasing age and weight.
Pathophysiology
Anatomically, the iliotibial band (ITB) is a continuation of the tendinous portion of the tensor fascia lata muscle with significant contributions from the gluteus maximus.[6][21][22] Distally, the ITB spans out and has attachments to the lateral border of the patella and lateral patellar retinaculum before its insertion on the Gerdy tubercle of the tibia. Anatomical dissections indicate a strong tendinous insertion at the lateral epicondyle of the femur with adipose tissue underneath (fat pad-like structure), and a ligamentous portion distally to the Gerdy tubercle.[21] During running, the posterior edge of the ITB impinges against the lateral epicondyle of the femur just after foot strike. This impingement zone occurs at, or at slightly less than, 30° of knee flexion. Repetitive irritation can lead to chronic inflammation, especially beneath the posterior fibers of the ITB, which are thought to be tighter against the lateral femoral epicondyle than the anterior fibers.
Male runners may exhibit kinematic faults such as increased hip internal rotation and knee varus, and weakness in the external rotator muscles of the hip.[13][23]
Studies of female runners have demonstrated external rotation of the femur in stance phase running, resulting in an internally rotated knee.[13][24] Female runners may exhibit increased hip adduction and knee internal rotation, and abnormal iliotibial band strain and strain rate.[25]
Knee internal rotation may be a factor in tightening the Gerdy tubercle portion of the ITB, adding to the tightening at the femoral epicondyle. Fatigue and segmental muscle coordination may be contributing factors to the excessive internal rotation at the knee and related issues at the hip.[20][26][Figure caption and citation for the preceding image starts]: Male runner with iliotibial band syndrome. The femur may or may not exhibit increased internal rotation. The investigators did not report on the mechanism of increased hip internal rotationBaker RL et al. Iliotibial band syndrome in runners: biomechanical implications and exercise interventions. Phys Med Rehabil Clin N Am. 2016 Feb;27(1):53-77; used with permission [Citation ends].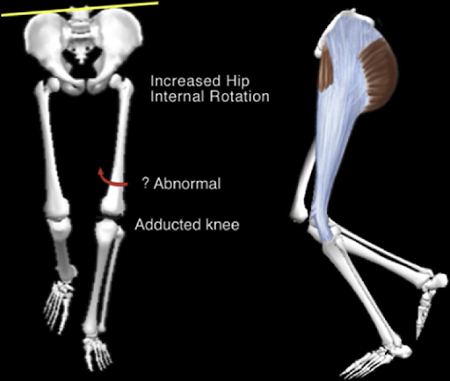 [Figure caption and citation for the preceding image starts]: Female runner with iliotibial band syndromeBaker RL et al. Iliotibial band syndrome in runners: biomechanical implications and exercise interventions. Phys Med Rehabil Clin N Am. 2016 Feb;27(1):53-77; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Female runner with iliotibial band syndromeBaker RL et al. Iliotibial band syndrome in runners: biomechanical implications and exercise interventions. Phys Med Rehabil Clin N Am. 2016 Feb;27(1):53-77; used with permission [Citation ends].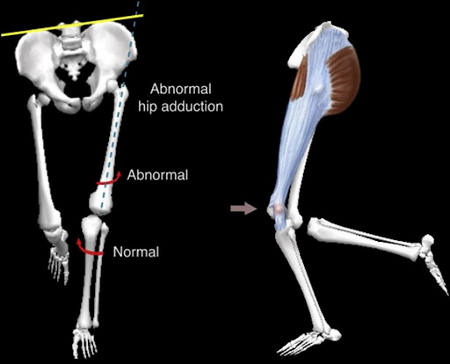 [Figure caption and citation for the preceding image starts]: Anatomy of iliotibial band. IT band, iliotibial band; Gluteus max, gluteus maximus; TFL, tensor fascia lataFrom the personal collection of Dr J.C. Mak [Citation ends].
[Figure caption and citation for the preceding image starts]: Anatomy of iliotibial band. IT band, iliotibial band; Gluteus max, gluteus maximus; TFL, tensor fascia lataFrom the personal collection of Dr J.C. Mak [Citation ends].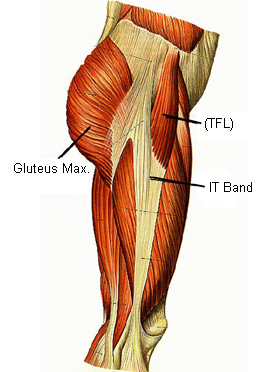 [Figure caption and citation for the preceding image starts]: Impingement zone occurring at around 30° of knee flexionFrom the personal collection of Dr J.C. Mak [Citation ends].
[Figure caption and citation for the preceding image starts]: Impingement zone occurring at around 30° of knee flexionFrom the personal collection of Dr J.C. Mak [Citation ends].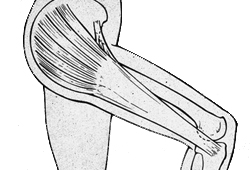
Use of this content is subject to our disclaimer