Approach
Clinical diagnosis of tendinopathy is based on careful palpation of the tendon in question. Presentation and exam features of tendinopathy at common sites are detailed below.
Imaging is not required to make a diagnosis but may assist in managing recalcitrant cases. It is important to view imaging studies in the context of their clinical findings.[30][31][32][33][Figure caption and citation for the preceding image starts]: MRI demonstrating calcific tendinopathy involving the distal central supraspinatusFrom the personal collection of James Wang, PhD [Citation ends]. [Figure caption and citation for the preceding image starts]: MRI demonstrating mild to moderate tendinopathy of the proximal centimeter of the patellar tendon, characterized by thickening and abnormal signal within the tendonFrom the personal collection of James Wang, PhD [Citation ends].
[Figure caption and citation for the preceding image starts]: MRI demonstrating mild to moderate tendinopathy of the proximal centimeter of the patellar tendon, characterized by thickening and abnormal signal within the tendonFrom the personal collection of James Wang, PhD [Citation ends].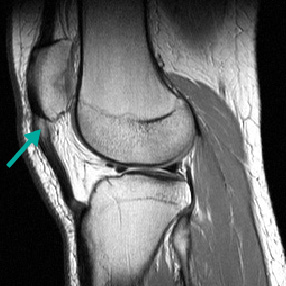
Plain radiographs may show calcium deposits in calcific tendinopathy, but are not useful in soft-tissue evaluation.
Ultrasound and magnetic resonance imaging (MRI) are generally not needed but may be utilized to demonstrate tendinosis in cases that are not straightforward.
Ultrasound is quick and inexpensive, but it is highly operator dependent.[34][35]
MRI allows evaluation of the surrounding structures and may aid in the diagnosis.
Rotator cuff tendinopathy
Presentation:
Common with overhead activities: throwing, swimming, and weightlifting.
Patients usually complain of a deep ache within the shoulder or pain with the normal range of motion.
Pertinent examination findings and maneuvers include:
Focal tenderness to palpation over Codman point (supraspinatus insertion onto the greater tuberosity)
Decreased supraspinatus strength with resisted abduction in the scapular plane (Jobe test)
Decreased infraspinatus and teres minor strength with resisted external rotation
Decreased subscapularis strength with resisted internal rotation
Impingement symptoms, which may be elicited with Neer and Hawkins maneuvers.[36][37][Figure caption and citation for the preceding image starts]: Impingement test: with hand in full pronation, passively raise shoulder in line of movement of scapula. Pain = positive testFrom the personal collection of James Wang, PhD [Citation ends].
 [Figure caption and citation for the preceding image starts]: Impingement test: with shoulder in 90º forward flexion, elbow in 90º flexion, apply downward pressure on the hand while stabilizing at the elbow. Pain = positive testFrom the personal collection of James Wang, PhD [Citation ends].
[Figure caption and citation for the preceding image starts]: Impingement test: with shoulder in 90º forward flexion, elbow in 90º flexion, apply downward pressure on the hand while stabilizing at the elbow. Pain = positive testFrom the personal collection of James Wang, PhD [Citation ends].
It is important to evaluate for rotator cuff tears, which are more common in patients >40 years of age. The diagnosis is based on the finding of rotator cuff weakness and/or impingement, which persists with subacromial local anesthesia, and if clinical doubt persists, confirmed by imaging with ultrasonography or MRI.[33]
Lateral epicondylitis (tennis elbow)
Presentation:
Patients complain of pain on the lateral aspect of their elbow, usually affecting the dominant side.
Typically a result of repetitive supination/pronation or flexion/extension with the elbow in near extension.
Making a fist and extending the wrist aggravate the pain.
Pertinent examination findings include:
Focal tenderness to palpation on the lateral epicondyle, focally prominent at the origin of the extensor carpi radialis brevis (ECRB) tendon. The disease mechanism is that of angiofibrotic dysplasia at ECRB tendon, not an inflammatory process.
Pain at the lateral epicondyle with resisted active wrist and long finger extension with the elbow in full extension. [Figure caption and citation for the preceding image starts]: Test for lateral epicondylitis: resisted wrist extension with elbow in full extension stresses the origin of the extensor carpi radialis brevis tendon and elicits pain at the lateral epicondyleFrom the personal collection of James Wang, PhD [Citation ends].

Medial epicondylitis (golfer's elbow)
Presentation:
Patients complain of medial elbow pain and a weak grip, usually affecting the dominant side.
Typically a result of repetitive pronation with the elbow in near extension.
Actively flexing the wrist aggravates the pain.
Pertinent examination findings include:
Focal tenderness to palpation on the medial epicondyle
Pain at the medial epicondyle with resisted forearm pronation and resisted palmar flexion [Figure caption and citation for the preceding image starts]: Test for medial epicondylitis: resisted forearm pronation and palmar flexion elicits pain at the medial epicondyleFrom the personal collection of James Wang, PhD [Citation ends].

Pain at the medial epicondyle with passive extension of the wrist and fingers.
Patellar tendinopathy (jumper's knee)
Presentation:
Common in jumping sports or activities that involve repetitive knee extension (e.g., volleyball, basketball, and soccer).
Patients present with an insidious onset of well-localized anterior knee pain located at the inferior pole of the patella.
Depending on the duration of symptoms, pain may occur after activity or during activity, or persist as a constant dull ache.
Pertinent exam findings include:
Focal tenderness to palpation of the patellar tendon at the inferior pole of the patella
Tenderness is worse when the knee is in full extension, as this allows palpation of the deep patellar tendon fibers, and decreases with knee flexion
Resisted knee extension also reproduces pain
Quadriceps weakness or atrophy may also be noted.
Quadriceps tendinopathy
Presentation:
Given the greater strength and increased vascularity of the quadriceps, tendinopathy in this area occurs less frequently than patellar tendinopathy.
Patients with quadriceps tendinopathy present with an insidious onset of anterior knee pain located at the superior pole of the patella.
Pertinent examination findings include:
Focal tenderness of the quadriceps tendon at the superior pole of the patella
Pain with resisted extension.
Achilles tendinopathy
Presentation:
Occurs in approximately 10% of runners.
Patients complain of insidious onset of heel pain often after a sudden increase in training intensity.
Other contributing factors include inappropriate footwear and change of running surface.
Pertinent examination findings include:
Localized tenderness in the mid portion of the Achilles tendon (2-6 cm above the insertion of the Achilles tendon insertion into the calcaneus, in the avascular zone)
Pain with resisted plantar flexion and passive dorsiflexion of the ankle
Crepitus
Tight hamstring-soleus complex.
It is important to rule-out Achilles tendon rupture by performing the Thompson test: with the patient prone, calf muscles are squeezed, which should intrinsically plantar flex the foot if the Achilles is intact.
Use of this content is subject to our disclaimer