Differentials
Common
Skull fracture (nonbasilar)
History
history of a high-velocity, direct impact to skull, a fall from height, or motor vehicle-related injury
Exam
evidence of scalp hematoma, crepitance, laceration or bony deformity; Glasgow Coma Scale score and focal deficits vary depending on underlying intracranial injury
1st investigation
- head CT (noncontrast):
will detect most skull fractures using the bone windows, and most underlying injury using the brain windows; compared with a suture, a fracture tends to be wider at the center and more narrowed at the ends, more than 3 mm in width, and runs in straight lines with angulated turns; a fracture can be linear or comminuted, and may be depressed through the inner table
More
Other investigations
- skull x-ray:
skull fracture
More
Base of skull fracture
History
history of high-velocity impact to the back of the head; may report clear fluid or blood draining from nose or ears; may report facial numbness, vertigo, or hearing deficits
Exam
post-auricular or periorbital ecchymosis, cerebrospinal fluid otorrhea or rhinorrhea, hemotympanum, cranial nerve VII and VIII deficits
1st investigation
- head CT (noncontrast):
will detect most skull fractures using the bone windows, and most underlying injury using the brain windows
More
Cerebral contusion
History
history of direct impact or acceleration/deceleration typically due to fall or motor vehicle-related injury; may have history of loss of consciousness
Exam
scalp trauma may be present; depending on severity; Glasgow Coma Scale score may be normal or decreased; if severe may have focal deficits, seizures, or signs of increased intracranial pressure
1st investigation
- head CT (noncontrast):
single or multiple parenchymal lesions, contusions commonly found on the frontal and temporal poles; approximately half are hemorrhagic: a focus of hyperdensity, surrounded by a hypodense area representative of edema; nonhemorrhagic lesions may be difficult to see on initial CT
More
Other investigations
- head MRI:
hemorrhagic contusions are hyperdense on T1-weighted imaging and hypodense on T2-weighted imaging; nonhemorrhagic lesions are hypodense on T1-weighted imaging and hyperdense on T2 imaging
More
Intracerebral hemorrhage
History
history of direct impact or rapid acceleration/deceleration typically due to fall or motor vehicle-related injury; witnesses may report lucid period, followed by progressive altered mental status
Exam
evidence of scalp trauma is common; seizures or focal neurologic deficits related to area of hemorrhage may be present; evidence of raised intracranial pressure and herniation: altered mental status, pupillary irregularity, extension to pain, respiratory irregularity, papilledema, fundal hemorrhage
1st investigation
- head CT (noncontrast):
hyperdense area of hemorrhage, surrounded by a hypodense area of edema
More
Other investigations
- head MRI:
acute hemorrhage is hyperdense on T1-weighted imaging and hypodense on T2-weighted imaging
More
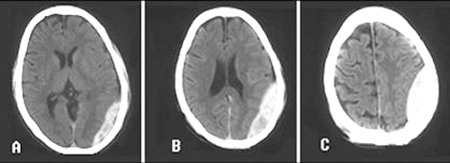
Subdural hematoma
History
history of direct impact or rapid acceleration/deceleration due to fall or motor vehicle-related injury; increased risk in patients with bleeding diathesis, anticoagulant medications, alcohol misuse; history of a fall is more common in patients with significant cerebral atrophy
Exam
scalp trauma may be present; focal neurologic deficits may develop, altered mental status depending on size of lesion; may have signs of increased intracranial pressure as hematoma size increases
1st investigation
- head CT (noncontrast):
characteristically crescent-shaped; blood does not cross the midline; in the setting of acute bleeding, areas of hypodense and hyperdense hematoma produce a swirling appearance
More
Other investigations
- head MRI:
T1-weighted MRI will appear as hypointense or isointense acutely; T2-weighted imaging will display SDH as hyperintense within the first few hours, progressing to a hypointensity over the ensuing week
More
Epidural hematoma
History
history of direct impact; patient may have had a lucid interval and then progressive deterioration of Glasgow Coma Scale
Exam
commonly scalp trauma over the temporal bone; focal neurologic deficits and progressive altered mental status
1st investigation
- head CT (noncontrast):
a hyperdense extra-axial lesion with smooth margins on CT; a lentiform appearance, forming a biconvex shape as blood pushes on the brain surface; blood does not cross suture lines; swirling areas of varying density indicate active bleeding
More
Other investigations
- MRI head:
can aid in the visualization of small EDH; signal intensity as similar to that seen with subdural hematoma
Intraventricular hemorrhage
History
history of direct impact or rapid acceleration/deceleration due to fall or motor vehicle-related injury; depending on degree of hydrocephaly, the patient may present with headache, vomiting, and ataxia or have progressed to an altered mental status
Exam
signs are due to secondary obstructive hydrocephalus and raised intracranial pressure: papilledema, fundal hemorrhage, decreased consciousness; signs of herniation include pupillary dilation, bilateral ptosis, impaired upgaze, extension to pain, and respiratory irregularity
1st investigation
- head CT (noncontrast):
blood in the ventricles will appear as hyperdense, commonly seen in the lateral ventricles; often other associated pathology; hydrocephalus may be seen
More
Other investigations
Traumatic subarachnoid hemorrhage
History
history of direct impact or rapid acceleration/deceleration, can occur due to a fall, but must rule out aneurysmal subarachnoid hemorrhage (SAH); aneurysmal SAH more likely if history of sudden onset of severe headache, meningeal symptoms, nausea; can be mild with minimal symptoms, or severe with symptoms of increased intracranial pressure (ICP): altered mental status, decreased consciousness
Exam
can be mild with minimal signs, or severe with signs of increased ICP: papilledema, fundal hemorrhage, altered mental status, decreased consciousness; signs of herniation: pupillary dilation, bilateral ptosis, impaired upgaze, extension to pain, respiratory irregularity
1st investigation
- head CT (noncontrast):
SAH on CT can be subtle; the basilar cisterns (suprasellar and quadrigeminal cisterns) should be inspected carefully for the presence of SAH, which appears hyperdense compared with cerebrospinal fluid
More
Other investigations
- CT angiography (CTA):
may be performed if etiology of SAH as traumatic is uncertain; visualizes potential vascular abnormalities or active bleeding sites
- head MRI:
SAH present
More - ECG:
nonspecific; ischemic changes in SAH include ST elevation or depression, abnormal T-wave morphology, prolonged QTc interval and U-waves.[142]
Penetrating injuries
History
history of high-velocity impact or missile injuries; symptoms depend on nature of injury and brain regions affected
Exam
should visualize and palpate for scalp defect, crepitance, obvious skull deformity or protruding foreign body; may have localizing neurologic deficits or seizures
1st investigation
- head CT (noncontrast):
the initial test of choice and can demonstrate the nature of the intracranial pathology and presence or absence of fractures and foreign bodies
More
Other investigations
- CT angiography:
may be required to evaluate further vascular injuries
- MRI:
contraindicated if there is any suspicion that a metal object has penetrated the skull
Diffuse axonal injury
History
history of direct impact or rapid acceleration/deceleration of head; depending on severity, may complain of headache or vomiting, or have had a rapid progressive deterioration of Glasgow Coma Scale and coma
Exam
patients with severe diffuse axonal injury (DAI) present with altered mental status or coma; classically have physical exam findings disproportionate to CT findings
1st investigation
- head CT (noncontrast):
initially normal in more than half of patients with DAI; should look for edema and petechial hemorrhage, at the gray/white junction, within the corpus callosum, and the brainstem
More
Other investigations
- MRI:
indicated when CT does not explain patient’s symptoms; more sensitive for microhemorrhage and edema
Mild traumatic brain injury
History
history of blunt trauma or acceleration/deceleration forces; can result in confusion, disorientation, or impaired consciousness, dysfunction of memory around the time of the injury, loss of consciousness lasting 30 minutes or less, posttraumatic amnesia for under 24 hours; can cause observed signs of neurologic or neuropsychologic dysfunction such as seizures acutely following injury; symptoms include headache, dizziness, fatigue, irritability, and poor concentration (typically referred to as "postconcussive symptoms")
Exam
Glasgow Coma Scale score of no worse than 13 after 30 minutes post injury or later upon presentation for health care; other transient neurologic abnormalities such as focal signs, seizure, and intracranial lesion not requiring surgery may be present
1st investigation
- head CT (noncontrast):
usually normal
More
Other investigations
- head MRI:
usually normal
More
Use of this content is subject to our disclaimer