Treatment is most commonly surgical and depends on the location of the fracture and whether it is displaced. Operative management results in a reduced length of hospital stay and improved rehabilitation compared with conservative methods (bed rest and traction), which are no longer recommended.[59]Handoll HH, Parker MJ. Conservative versus operative treatment for hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000337.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000337.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/18646065?tool=bestpractice.com
Multiple guidelines recommend early surgery following medical assessment.[60]Mak JC, Cameron ID, March LM; National Health and Medical Research Council (Australia). Evidence-based guidelines for the management of hip fractures in older persons: an update. Med J Aust. 2010 Jan 4;192(1):37-41.
http://www.ncbi.nlm.nih.gov/pubmed/20047547?tool=bestpractice.com
[61]Khan SK, Kalra S, Khanna A, et al. Timing of surgery for hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009 Jul;40(7):692-7.
http://www.ncbi.nlm.nih.gov/pubmed/19450802?tool=bestpractice.com
[62]National Institute for Health and Care Excellence. Hip fracture: management. Jan 2023 [internet publication].
https://www.nice.org.uk/guidance/cg124
Surgery within 24-48 hours of admission may be associated with better outcomes.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
The American Academy of Orthopaedic Surgeons (AAOS) recommends that patients with open fractures are brought to the operating room for debridement and irrigation as soon as reasonable, and ideally within 24 hours post injury.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
Meta-analyses report reduced mortality and reduced complications following early surgery.[63]Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ. 2010 Oct 19;182(15):1609-16.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2952007
http://www.ncbi.nlm.nih.gov/pubmed/20837683?tool=bestpractice.com
[64]Moja L, Piatti A, Pecoraro V, et al. Timing matters in hip fracture surgery: patients operated within 48 hours have better outcomes - a meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3463569
http://www.ncbi.nlm.nih.gov/pubmed/23056256?tool=bestpractice.com
In one large retrospective cohort study, hip fracture surgery within 24 hours was associated with significantly reduced risk of 30-day mortality compared with surgery after 24 hours (5.8% vs. 6.5%, respectively).[65]Pincus D, Ravi B, Wasserstein D, et al. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. 2017 Nov 28;318(20):1994-2003.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5820694
http://www.ncbi.nlm.nih.gov/pubmed/29183076?tool=bestpractice.com
Accelerated surgery (median time from hip fracture diagnosis to surgery of 6 hours) did not significantly reduce risk of mortality or a composite of major complications compared with standard care (surgery within 24 hours) in one large randomized controlled trial (RCT).[66]HIP ATTACK Investigators. Accelerated surgery versus standard care in hip fracture (HIP ATTACK): an international, randomised, controlled trial. Lancet. 2020 Feb 29;395(10225):698-708.
http://www.ncbi.nlm.nih.gov/pubmed/32050090?tool=bestpractice.com
Venous thromboembolism prophylaxis
Guidelines from the AAOS strongly recommend venous thromboembolism (VTE) prophylaxis in all patients ages 65 years or older. There are significant established risk factors for VTE in these patients, including age, presence of hip fracture, major surgery, delays to surgery, and the potential serious consequences of failure to provide prophylaxis.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
This recommendation was based on data from six moderate-quality studies and four low-quality studies that showed the risk of deep vein thrombosis (DVT) was significantly less with VTE prophylaxis than with control. Most general complications were not significantly different between treatment groups and there was some evidence that mortality was less with prophylaxis when compared with control groups.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Other guidelines agree that some form of prophylaxis is necessary regardless of the patient's age; however, there is no consensus on choice of agent or duration.[67]Falck-Ytter Y, Francis CW, Johanson NA, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012 Feb;141(2 suppl):e278S-325S.
http://journal.chestnet.org/article/S0012-3692(12)60126-3/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/22315265?tool=bestpractice.com
[68]Anderson DR, Morgano GP, Bennett C, et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019 Dec 10;3(23):3898-44.
https://www.doi.org/10.1182/bloodadvances.2019000975
http://www.ncbi.nlm.nih.gov/pubmed/31794602?tool=bestpractice.com
[69]National Institute for Health and Care Excellence. Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism. August 2019 [internet publication].
https://www.nice.org.uk/guidance/NG89
Total hip arthroplasty and open reduction and internal fixation of hip fractures, and surgery due to major trauma, are among the orthopedic procedures with the highest DVT risk.[70]ICM-VTE General Delegates. Recommendations from the ICM-VTE: general. J Bone Joint Surg Am. 2022 Mar 16;104(suppl 1):4-162.
https://journals.lww.com/jbjsjournal/fulltext/2022/03161/recommendations_from_the_icm_vte__general.2.aspx
http://www.ncbi.nlm.nih.gov/pubmed/35315607?tool=bestpractice.com
With contemporary surgical protocols the prevalence of VTE after total hip arthroplasty has been reported to be up to 22%, using venography as a diagnostic method, even with pharmacologic prophylaxis.[71]Verhamme P, Yi BA, Segers A, et al. Abelacimab for prevention of venous thromboembolism. N Engl J Med. 2021 Aug 12;385(7):609-17.
https://www.nejm.org/doi/10.1056/NEJMoa2105872
http://www.ncbi.nlm.nih.gov/pubmed/34297496?tool=bestpractice.com
See Venous thromboembolism (VTE) prophylaxis.
Preoperative antibiotic therapy
Early delivery of antibiotics is suggested to lower the risk of deep infection in the setting of open fracture in major extremity trauma.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
Results from meta-analyses suggest that prophylactic antibiotics significantly reduce the risk of postoperative superficial and deep wound infection (relative risk reduction of 45% to 60%, depending on analysis).[72]Southwell-Keely JP, Russo RR, March L, et al. Antibiotic prophylaxis in hip fracture surgery: a metaanalysis. Clin Orthop Relat Res. 2004 Feb;(419):179-84.
https://journals.lww.com/clinorthop/Fulltext/2004/02000/Antibiotic_Prophylaxis_in_Hip_Fracture_Surgery__A.29.aspx
http://www.ncbi.nlm.nih.gov/pubmed/15021151?tool=bestpractice.com
[73]Gillespie WJ, Walenkamp G. Antibiotic prophylaxis for surgery for proximal femoral and other closed long bone fractures. Cochrane Database Syst Rev. 2010 Mar 17;(3):CD000244.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000244.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/20238310?tool=bestpractice.com
The use of multiple antibiotics or antibiotic use for more than 24 hours had no further effect on postoperative infection.
Most trials used a regimen either 1 hour prior to induction or at induction, and most antibiotics delivered were intravenous and either a first- or second-generation cephalosporin.[72]Southwell-Keely JP, Russo RR, March L, et al. Antibiotic prophylaxis in hip fracture surgery: a metaanalysis. Clin Orthop Relat Res. 2004 Feb;(419):179-84.
https://journals.lww.com/clinorthop/Fulltext/2004/02000/Antibiotic_Prophylaxis_in_Hip_Fracture_Surgery__A.29.aspx
http://www.ncbi.nlm.nih.gov/pubmed/15021151?tool=bestpractice.com
[73]Gillespie WJ, Walenkamp G. Antibiotic prophylaxis for surgery for proximal femoral and other closed long bone fractures. Cochrane Database Syst Rev. 2010 Mar 17;(3):CD000244.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000244.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/20238310?tool=bestpractice.com
In patients with major extremity trauma undergoing surgery, the AAOS strongly recommends that antibiotic prophylaxis with systemic cefazolin or clindamycin be administered, except for type III (and possibly type II) open fractures, for which additional gram-negative coverage (e.g., piperacillin/tazobactam) is preferred.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
However, local sensitivities and protocols should be followed for antibiotic selection.
In patients with major extremity trauma undergoing surgery, local antibiotic prophylactic strategies such as vancomycin powder, tobramycin-impregnated beads, or gentamicin-covered nails may be beneficial, when available.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
One systematic review and meta-analysis suggests that both single-dose and multi-dose antibiotic prophylaxis reduce the risk of deep surgical site infection, with similar effect size.[73]Gillespie WJ, Walenkamp G. Antibiotic prophylaxis for surgery for proximal femoral and other closed long bone fractures. Cochrane Database Syst Rev. 2010 Mar 17;(3):CD000244.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000244.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/20238310?tool=bestpractice.com
Intracapsular (femoral neck) fracture: undisplaced
Treatment in most instances is internal fixation with a dynamic hip screw, or multiple cannulated screws, when the wound is determined to be clean.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
[60]Mak JC, Cameron ID, March LM; National Health and Medical Research Council (Australia). Evidence-based guidelines for the management of hip fractures in older persons: an update. Med J Aust. 2010 Jan 4;192(1):37-41.
http://www.ncbi.nlm.nih.gov/pubmed/20047547?tool=bestpractice.com
One Cochrane review comparing screws and fixed angle plates found there may be little or no difference in functional status, quality of life, 1-year mortality, or unplanned reoperations.[74]Lewis SR, Macey R, Eardley WG, et al. Internal fixation implants for intracapsular hip fractures in older adults. Cochrane Database Syst Rev. 2021 Mar 9;3(3):CD013409.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013409.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/33687067?tool=bestpractice.com
One RCT in patients with undisplaced (66%) or displaced (34%) low-energy femoral neck fracture determined that reoperation rates at 24 months were similar for the two surgical fixation methods.[75]Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017 Apr 15;389(10078):1519-27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5597430
http://www.ncbi.nlm.nih.gov/pubmed/28262269?tool=bestpractice.com
Secondary analysis of this RCT, and results from a retrospective cohort study, reported an association between preoperative posterior tilt ≥20° and increased risk of subsequent arthroplasty in patients with undisplaced or minimally displaced femoral neck fractures (Garden I-II). Arthroplasty may, therefore, be a superior initial treatment option to internal fixation for patients with posterior tilt ≥20°.[76]Okike K, Udogwu UN, Isaac M, et al. Not all Garden-I and II femoral neck fractures in the elderly should be fixed: effect of posterior tilt on rates of subsequent arthroplasty. J Bone Joint Surg Am. 2019 Oct 16;101(20):1852-9.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7406148
http://www.ncbi.nlm.nih.gov/pubmed/31626010?tool=bestpractice.com
[77]Sjöholm P, Otten V, Wolf O, et al. Posterior and anterior tilt increases the risk of failure after internal fixation of Garden I and II femoral neck fracture. Acta Orthop. 2019 Dec;90(6):537-41.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6844400
http://www.ncbi.nlm.nih.gov/pubmed/31269853?tool=bestpractice.com
Intracapsular (femoral neck) fracture: displaced
Surgical approach to repair of displaced femoral neck fracture may be influenced by several factors, including patient age.
For patients ages younger than 65 years, most surgeons favor urgent (<12-24 hours from injury) open reduction and internal fixation due in part to a potential increased risk of avascular necrosis to the femoral head.[78]Jain R, Koo M, Kreder HJ, et al. Comparison of early and delayed fixation of subcapital hip fractures in patients sixty years of age or less. J Bone Joint Surg Am. 2002 Sep;84-A(9):1605-12.
http://www.ncbi.nlm.nih.gov/pubmed/12208917?tool=bestpractice.com
[79]Dedrick DK, Mackenzie JR, Burney RE. Complications of femoral neck fracture in young adults. J Trauma. 1986 Oct;26(10):932-7.
http://www.ncbi.nlm.nih.gov/pubmed/3773004?tool=bestpractice.com
However, evidence is conflicting regarding rates of avascular necrosis and timing of surgery.[80]Duckworth AD, Bennet SJ, Aderinto J, et al. Fixation of intracapsular fractures of the femoral neck in young patients: risk factors for failure. J Bone Joint Surg Br. 2011 Jun;93(6):811-6.
http://www.ncbi.nlm.nih.gov/pubmed/21586782?tool=bestpractice.com
[81]Lowe JA, Crist BD, Bhandari M, et al. Optimal treatment of femoral neck fractures according to patient's physiologic age: an evidence-based review. Orthop Clin North Am. 2010 Apr;41(2):157-66.
http://www.ncbi.nlm.nih.gov/pubmed/20399355?tool=bestpractice.com
For patients 65 years and older with unstable (displaced) femoral neck fractures, the AAOS strongly recommends arthroplasty over fixation.
Randomized trials comparing arthroplasty (hemi- and/or total hip arthroplasty) with internal fixation have consistently reported better outcomes (reoperation rate, pain scores, functional status, and/or complication rate) for arthroplasty.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[82]Lu Q, Tang G, Zhao X, et al. Hemiarthroplasty versus internal fixation in super-aged patients with undisplaced femoral neck fractures: a 5-year follow-up of randomized controlled trial. Arch Orthop Trauma Surg. 2017 Jan;137(1):27-35.
http://www.ncbi.nlm.nih.gov/pubmed/27837321?tool=bestpractice.com
[83]Støen RØ, Lofthus CM, Nordsletten L, et al. Randomized trial of hemiarthroplasty versus internal fixation for femoral neck fractures: no differences at 6 years. Clin Orthop Relat Res. 2014 Jan;472(1):360-7.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3889441
http://www.ncbi.nlm.nih.gov/pubmed/23975250?tool=bestpractice.com
[84]Parker MJ, Pryor G, Gurusamy K. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures: a long-term follow-up of a randomised trial. Injury. 2010 Apr;41(4):370-3.
http://www.ncbi.nlm.nih.gov/pubmed/19879576?tool=bestpractice.com
Evidence from meta-analyses suggests that mortality at 1 year did not differ; arthroplasty was associated with greater operative time, and significantly increased the risk of infection and blood loss.[85]Bhandari M, Devereaux PJ, Swiontkowski MF, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck: a meta-analysis. J Bone Joint Surg Am. 2003 Sep;85-A(9):1673-81.
http://www.ncbi.nlm.nih.gov/pubmed/12954824?tool=bestpractice.com
[86]Parker MJ, Gurusamy K. Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD001708.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001708.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/17054139?tool=bestpractice.com
In appropriately selected patients aged 65 years and older with unstable (displaced) femoral neck fractures, there may be a functional benefit to total hip arthroplasty over hemiarthroplasty at the risk of increasing complications.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Several studies demonstrate a small functional outcome benefit and fewer reoperations in patients who received total hip arthroplasty. However, the effect size in these studies is small and mortality rates were largely unaffected within the first 4 years after treatment.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[87]Lewis DP, Wæver D, Thorninger R, et al. Hemiarthroplasty vs total hip arthroplasty for the management of displaced neck of femur fractures: a systematic review and meta-analysis. J Arthroplasty. 2019 Aug;34(8):1837-43.
http://www.ncbi.nlm.nih.gov/pubmed/31060915?tool=bestpractice.com
[88]Burgers PT, Van Geene AR, Van den Bekerom MP, et al. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures in the healthy elderly: a meta-analysis and systematic review of randomized trials. Int Orthop. 2012 Aug;36(8):1549-60.
http://rd.springer.com/article/10.1007%2Fs00264-012-1569-7/fulltext.html
http://www.ncbi.nlm.nih.gov/pubmed/22623062?tool=bestpractice.com
[89]HEALTH Investigators; Bhandari M, Einhorn TA, Guyatt G, et al. Total hip arthroplasty or hemiarthroplasty for hip fracture. N Engl J Med. 2019 Dec 5;381(23):2199-208.
https://www.nejm.org/doi/10.1056/NEJMoa1906190
http://www.ncbi.nlm.nih.gov/pubmed/31557429?tool=bestpractice.com
[90]Sharma V, Awasthi B, Kumar K, et al. Outcome analysis of hemiarthroplasty vs. total hip replacement in displaced femoral neck fractures in the elderly. J Clin Diagn Res. 2016 May;10(5):RC11-3.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4948492
http://www.ncbi.nlm.nih.gov/pubmed/27437316?tool=bestpractice.com
The AAOS also notes that patient exclusion criteria in some of these studies reflect the general bias among surgeons toward performing total hip arthroplasty in patients who are higher functioning and more likely to be independent community ambulators.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
The AAOS, therefore, recommends that cautious decision-making around total hip arthroplasty versus hemiarthroplasty for lower functioning patients may be justified considering the bias and risk for complications.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Despite the apparent benefits of total hip arthroplasty (reflected in some US and UK guideline recommendations for total hip arthroplasty in ambulatory patients with displaced femoral neck fractures), many surgeons prefer hemiarthroplasty for older patients with displaced femoral neck fracture.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[62]National Institute for Health and Care Excellence. Hip fracture: management. Jan 2023 [internet publication].
https://www.nice.org.uk/guidance/cg124
[91]Bhandari M, Devereaux PJ, Tornetta P 3rd, et al. Operative management of displaced femoral neck fractures in elderly patients: an international survey. J Bone Joint Surg Am. 2005 Sep;87(9):2122-30.
http://www.ncbi.nlm.nih.gov/pubmed/16140828?tool=bestpractice.com
[92]Woon CYL, Moretti VM, Schwartz BE, et al. Total hip arthroplasty and hemiarthroplasty: US national trends in the treatment of femoral neck fractures. Am J Orthop (Belle Mead NJ). 2017 Nov/Dec;46(6):E474-8.
http://www.ncbi.nlm.nih.gov/pubmed/29309466?tool=bestpractice.com
[93]Iorio R, Schwartz B, Macaulay W, et al. Surgical treatment of displaced femoral neck fractures in the elderly: a survey of the American Association of Hip and Knee Surgeons. J Arthroplasty. 2006 Dec;21(8):1124-33.
http://www.ncbi.nlm.nih.gov/pubmed/17162171?tool=bestpractice.com
Ambulatory status and decreased risk of dislocation (instability) have been cited as factors for choosing hemiarthroplasty.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[93]Iorio R, Schwartz B, Macaulay W, et al. Surgical treatment of displaced femoral neck fractures in the elderly: a survey of the American Association of Hip and Knee Surgeons. J Arthroplasty. 2006 Dec;21(8):1124-33.
http://www.ncbi.nlm.nih.gov/pubmed/17162171?tool=bestpractice.com
Surgeon volume is associated with reduced risk for dislocation and revision in patients undergoing primary total hip arthroplasty.[94]Ravi B, Jenkinson R, Austin PC, et al. Relation between surgeon volume and risk of complications after total hip arthroplasty: propensity score matched cohort study. BMJ. 2014 May 23;348:g3284.
https://www.bmj.com/content/348/bmj.g3284.long
http://www.ncbi.nlm.nih.gov/pubmed/24859902?tool=bestpractice.com
Most surgeons favor hemiarthroplasty for patients over 80 years of age.[21]National Institutes of Health (NIH). Osteoporosis prevention, diagnosis, and therapy. NIH Consens Statement. 2000 Mar 27-29;17(1):1-45.
http://www.ncbi.nlm.nih.gov/pubmed/11525451?tool=bestpractice.com
[91]Bhandari M, Devereaux PJ, Tornetta P 3rd, et al. Operative management of displaced femoral neck fractures in elderly patients: an international survey. J Bone Joint Surg Am. 2005 Sep;87(9):2122-30.
http://www.ncbi.nlm.nih.gov/pubmed/16140828?tool=bestpractice.com
The AAOS guideline states that unipolar or bipolar hemiarthroplasty in patients 65 years and older can be equally beneficial.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Patient preference
In a decision board study, when patients were asked which procedure they would prefer if they had a displaced neck of femur fracture, 93% of participants chose a total hip replacement over a hemiarthroplasty as their treatment of choice. Important factors in their decision were the perception of a greater walking distance, less residual pain, and risk of reoperation.[95]Alolabi N, Alolabi B, Mundi R, et al. Surgical preferences of patients at risk of hip fractures: hemiarthroplasty versus total hip arthroplasty. BMC Musculoskelet Disord. 2011 Dec 23;12:289.
http://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/1471-2474-12-289
http://www.ncbi.nlm.nih.gov/pubmed/22196211?tool=bestpractice.com
Cemented versus uncemented hemiarthroplasty
Guidelines recommend the use of cemented femoral stems in patients undergoing arthroplasty for femoral neck fracture based upon studies that demonstrated improved outcomes (decreased pain and increased mobility) when cemented stems were compared with first-generation uncemented stems (e.g., Austin-Moore prosthesis).[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[96]Parker MI, Pryor G, Gurusamy K. Cemented versus uncemented hemiarthroplasty for intracapsular hip fractures: a randomised controlled trial in 400 patients. J Bone Joint Surg Br. 2010 Jan;92(1):116-22.
http://www.ncbi.nlm.nih.gov/pubmed/20044689?tool=bestpractice.com
Subsequent trials, systematic reviews, and meta-analyses confirmed these findings, or reported no difference between cemented and uncemented femoral stems.[97]Inngul C, Blomfeldt R, Ponzer S, et al. Cemented versus uncemented arthroplasty in patients with a displaced fracture of the femoral neck: a randomised controlled trial. Bone Joint J. 2015 Nov;97-B(11):1475-80.
http://www.ncbi.nlm.nih.gov/pubmed/26530648?tool=bestpractice.com
[98]Deangelis JP, Ademi A, Staff I, et al. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: a prospective randomized trial with early follow-up. J Orthop Trauma. 2012 Mar;26(3):135-40.
http://www.ncbi.nlm.nih.gov/pubmed/22198652?tool=bestpractice.com
[99]Ning GZ, Li YL, Wu Q, et al. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: an updated meta-analysis. Eur J Orthop Surg Traumatol. 2014 Jan;24(1):7-14.
http://www.ncbi.nlm.nih.gov/pubmed/23412274?tool=bestpractice.com
[100]Luo X, He S, Li Z, et al. Systematic review of cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures in older patients. Arch Orthop Trauma Surg. 2012 Apr;132(4):455-63.
http://www.ncbi.nlm.nih.gov/pubmed/22160512?tool=bestpractice.com
One 2017 systematic review and meta-analysis of contemporary stems for displaced fracture of the femoral neck found that cemented femoral stems were associated with fewer implant-related complications than uncemented stems, but mortality did not differ between the two fixation methods.[101]Veldman HD, Heyligers IC, Grimm B, et al. Cemented versus cementless hemiarthroplasty for a displaced fracture of the femoral neck: a systematic review and meta-analysis of current generation hip stems. Bone Joint J. 2017 Apr;99-B(4):421-31.
http://www.ncbi.nlm.nih.gov/pubmed/28385929?tool=bestpractice.com
A small, single-center RCT of patients with femoral neck fracture (n=141) treated with arthroplasty suggested that cemented stems provide improved functional outcome scores compared with modern uncemented femoral stems.[97]Inngul C, Blomfeldt R, Ponzer S, et al. Cemented versus uncemented arthroplasty in patients with a displaced fracture of the femoral neck: a randomised controlled trial. Bone Joint J. 2015 Nov;97-B(11):1475-80.
http://www.ncbi.nlm.nih.gov/pubmed/26530648?tool=bestpractice.com
A larger, multicenter RCT to compare cemented hemiarthroplasty with contemporary modern hydroxyapatite-coated uncemented hemiarthroplasty is ongoing.[102]Fernandez MA, Achten J, Lerner RG, et al. Randomised controlled trial comparing hydroxyapatite coated uncemented hemiarthroplasty with cemented hemiarthroplasty for the treatment of displaced intracapsular hip fractures: a protocol for the WHITE 5 study. BMJ Open. 2019 Dec 9;9(12):e033957.
https://bmjopen.bmj.com/content/9/12/e033957.long
http://www.ncbi.nlm.nih.gov/pubmed/31822548?tool=bestpractice.com
One Cochrane review identified moderate-certainty evidence of a benefit with cemented hemiarthroplasty consistent with clinically small-to-large differences in health-related quality of life and reduction in the risk of mortality at 12 months, but little or no difference in performance of activities of daily living and independent mobility. The risks of most adverse events were similar. However, cemented hemiarthroplasties led to fewer periprosthetic fractures intraoperatively and postoperatively, but had a higher risk of pulmonary embolus.[103]Lewis SR, Macey R, Parker MJ, et al. Arthroplasties for hip fracture in adults. Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013410.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013410.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/35156194?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Anteroposterior pelvic radiograph showing a left intracapsular fracture fixed with a sliding hip screw constructFrom the collection of Bradley A. Petrisor, MSc, MD, FRCSC and Mohit Bhandari, MD, MSc, FRCSC [Citation ends].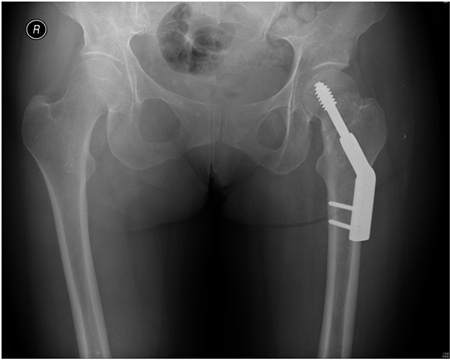
Extracapsular (intertrochanteric) fracture
Undisplaced
Displaced (stable or unstable)
Operative management includes internal fixation with either a dynamic hip screw or a cephalomedullary (intramedullary) nail in patients with stable intertrochanteric fractures when the wound is determined to be clean.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[Figure caption and citation for the preceding image starts]: Intramedullary nail (cephalomedullary) for the treatment of an unstable intertrochanteric fractureFrom the collection of Bradley A. Petrisor, MSc, MD, FRCSC and Mohit Bhandari, MD, MSc, FRCSC [Citation ends].
Choice of device
Overall, trends in management have led to cephalomedullary nails being selected more commonly (68%) than sliding hip screws (19%) for the management of both stable and unstable intertrochanteric hip fractures, with ease of surgical technique being the most commonly cited reason.[104]Niu E, Yang A, Harris AH, et al. Which fixation device is preferred for surgical treatment of intertrochanteric hip fractures in the United States? A survey of orthopaedic surgeons. Clin Orthop Relat Res. 2015 Nov;473(11):3647-55.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586189
http://www.ncbi.nlm.nih.gov/pubmed/26208608?tool=bestpractice.com
One RCT suggested a trend towards improved early mobility (<12 months) in patients treated with cephalomedullary nails.[105]Parker MJ, Cawley S. Sliding hip screw versus the Targon PFT nail for trochanteric hip fractures: a randomised trial of 400 patients. Bone Joint J. 2017 Sep;99-B(9):1210-5.
http://www.ncbi.nlm.nih.gov/pubmed/28860402?tool=bestpractice.com
Larger cohort studies indicate that there may be a higher rate of 30-day mortality, and bleeding, respiratory, and clotting complications in those treated with a cephalomedullary device.[106]Pandarinath R, Amdur R, DeBritz JN, et al. Comparison of short-term complication rates between cephalomedullary hip screw devices and sliding hip screws: an analysis of the National Surgical Quality Improvement Program Database. J Am Acad Orthop Surg. 2018 Dec 1;26(23):845-51.
http://www.ncbi.nlm.nih.gov/pubmed/30252786?tool=bestpractice.com
This, in combination with a lack of long-term differences, indicates that cephalomedullary implants are likely being overutilized in lieu of sliding hip screws, with perceived ease of surgical technique and nonclinically significant shorter surgical times being the major drivers of implant selection.
Guidelines from the AAOS strongly recommend use of either a sliding hip screw or a cephalomedullary device in patients with stable intertrochanteric fractures.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Fixation with either an extramedullary or intramedullary implant show similar clinical outcomes.[107]Cai L, Wang T, Di L, et al. Comparison of intramedullary and extramedullary fixation of stable intertrochanteric fractures in the elderly: a prospective randomised controlled trial exploring hidden perioperative blood loss. BMC Musculoskelet Disord. 2016 Nov 15;17(1):475.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5109735
http://www.ncbi.nlm.nih.gov/pubmed/27846888?tool=bestpractice.com
[108]Varela-Egocheaga JR, Iglesias-Colao R, Suárez-Suárez MA, et al. Minimally invasive osteosynthesis in stable trochanteric fractures: a comparative study between Gotfried percutaneous compression plate and Gamma 3 intramedullary nail. Arch Orthop Trauma Surg. 2009 Oct;129(10):1401-7.
http://www.ncbi.nlm.nih.gov/pubmed/19672606?tool=bestpractice.com
Results from early trials suggested that intramedullary nails were associated with increased risk of intra- or postoperative femoral fracture in patients with stable or unstable extracapsular proximal femoral fracture (compared with dynamic hip screws).[109]Lewis SR, Macey R, Gill JR, et al. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database Syst Rev. 2022 Jan 26;1(1):CD000093.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000093.pub6/full
http://www.ncbi.nlm.nih.gov/pubmed/35080771?tool=bestpractice.com
This was largely due to a mismatch between intramedullary nail geometry and femoral anatomy, with the implant having a lower radius of curvature than that of the femoral bow. Subsequent-generation intramedullary nails have addressed this by adjusting nail designs for improved femoral fit, and are less likely to be associated with periprosthetic fractures.[96]Parker MI, Pryor G, Gurusamy K. Cemented versus uncemented hemiarthroplasty for intracapsular hip fractures: a randomised controlled trial in 400 patients. J Bone Joint Surg Br. 2010 Jan;92(1):116-22.
http://www.ncbi.nlm.nih.gov/pubmed/20044689?tool=bestpractice.com
Multiple studies including prospective cohorts and RCTs continue to show equivalent outcomes between the two fixation options with respect to mortality, rates of failure, need for reoperation, length of stay, complications, and mobility at 1 year.[105]Parker MJ, Cawley S. Sliding hip screw versus the Targon PFT nail for trochanteric hip fractures: a randomised trial of 400 patients. Bone Joint J. 2017 Sep;99-B(9):1210-5.
http://www.ncbi.nlm.nih.gov/pubmed/28860402?tool=bestpractice.com
[109]Lewis SR, Macey R, Gill JR, et al. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database Syst Rev. 2022 Jan 26;1(1):CD000093.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000093.pub6/full
http://www.ncbi.nlm.nih.gov/pubmed/35080771?tool=bestpractice.com
[110]Whale CS, Hulet DA, Beebe MJ, et al. Cephalomedullary nail versus sliding hip screw for fixation of AO 31 A1/2 intertrochanteric femoral fracture: a 12-year comparison of failure, complications, and mortality. Curr Orthop Pract. Nov-Dec 2016;27(6):604-13.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5364496
http://www.ncbi.nlm.nih.gov/pubmed/28348717?tool=bestpractice.com
[111]Warren JA, Sundaram K, Hampton R, et al. Cephalomedullary nailing versus sliding hip screws for Intertrochanteric and basicervical hip fractures: a propensity-matched study of short-term outcomes in over 17,000 patients. Eur J Orthop Surg Traumatol. 2020 Feb;30(2):243-50.
http://www.ncbi.nlm.nih.gov/pubmed/31486944?tool=bestpractice.com
One prospective randomized trial found no difference in functional outcome, hospital stay, fracture collapse, or mortality between a cephalomedullary nail and an extramedullary sliding hip screw and plate device that offers two points of fixation into the femoral head.[108]Varela-Egocheaga JR, Iglesias-Colao R, Suárez-Suárez MA, et al. Minimally invasive osteosynthesis in stable trochanteric fractures: a comparative study between Gotfried percutaneous compression plate and Gamma 3 intramedullary nail. Arch Orthop Trauma Surg. 2009 Oct;129(10):1401-7.
http://www.ncbi.nlm.nih.gov/pubmed/19672606?tool=bestpractice.com
The AAOS strongly recommends that patients with unstable intertrochanteric fractures should be treated with a cephalomedullary device.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
In patients with subtrochanteric or reverse obliquity fractures, the AAOS recommends a cephalomedullary device.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
This recommendation is on the basis of apparent treatment benefit with lower general complication rate and wound infection rates, improved mobility, and decreased limb shortening.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[112]Miedel R, Ponzer S, Törnkvist H, et al. The standard Gamma nail or the Medoff sliding plate for unstable trochanteric and subtrochanteric fractures. A randomised, controlled trial. J Bone Joint Surg Br. 2005 Jan;87(1):68-75.
http://www.ncbi.nlm.nih.gov/pubmed/15686240?tool=bestpractice.com
Supportive care
Assess patients for volume depletion and administer intravenous fluids according to local protocols.[113]Miller TE, Myles PS. Perioperative fluid therapy for major surgery. Anesthesiology. 2019 May;130(5):825-32.
https://www.doi.org/10.1097/ALN.0000000000002603
http://www.ncbi.nlm.nih.gov/pubmed/30789364?tool=bestpractice.com
Postoperative supportive care includes optimizing pain control, nutrition, physical therapy, and multidisciplinary rehabilitation programs for postoperative mobility.[114]Cameron ID. Coordinated multidisciplinary rehabilitation after hip fracture. Disabil Rehabil. 2005 Sep 30-Oct 15;27(18-19):1081-90.
http://www.ncbi.nlm.nih.gov/pubmed/16315427?tool=bestpractice.com
The AAOS suggests a blood transfusion threshold of no higher than 8 g/dL in asymptomatic postoperative hip fracture patients ages 65 years and older to decrease the likelihood of transfusion-associated complications and cost; other guidelines recommend the same transfusion threshold (<8 g/dL) regardless of patient age.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[115]Mueller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: recommendations from the 2018 Frankfurt Consensus Conference. JAMA. 2019 Mar 12;321(10):983-97.
http://www.ncbi.nlm.nih.gov/pubmed/30860564?tool=bestpractice.com
[116]Carson JL, Stanworth SJ, Guyatt G, et al. Red blood cell transfusion: 2023 AABB international guidelines. JAMA. 2023 Nov 21;330(19):1892-902.
http://www.ncbi.nlm.nih.gov/pubmed/37824153?tool=bestpractice.com
Overall clinical context and individual patient factors should be considered.[116]Carson JL, Stanworth SJ, Guyatt G, et al. Red blood cell transfusion: 2023 AABB international guidelines. JAMA. 2023 Nov 21;330(19):1892-902.
http://www.ncbi.nlm.nih.gov/pubmed/37824153?tool=bestpractice.com
The AAOS strongly recommends tranexamic acid to reduce blood loss and blood transfusion in patients with hip fractures.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Postoperative pain management
Analgesia can be delivered with nerve blocks (i.e., fascia iliaca compartment block), patient-controlled analgesia, or prescription of routine opioids or epidural analgesia.[117]Foss NB, Kristensen MT, Kristensen BB, et al. Effect of postoperative epidural analgesia on rehabilitation and pain after hip fracture surgery: a randomized, double-blind, placebo-cotrolled trial. Anesthesiology. 2005 Jun;102(6):1197-204.
http://www.ncbi.nlm.nih.gov/pubmed/15915033?tool=bestpractice.com
Requirements may be related in part to the particular surgery that was done (e.g., dynamic hip screw, cephalomedullary device, hemiarthroplasty, etc).[118]Foss NB, Kristensen MT, Palm H, et al. Postoperative pain after hip fracture is procedure specific. Br J Anaesth. 2009 Jan;102(1):111-6.
https://academic.oup.com/bja/article/102/1/111/230174/Postoperative-pain-after-hip-fracture-is-procedure
http://www.ncbi.nlm.nih.gov/pubmed/19059921?tool=bestpractice.com
High-quality evidence indicates that pre- or postoperative peripheral nerve blocks for hip fractures reduce pain on movement within 30 minutes after block placement. Moderate-quality evidence shows reduced risk for pneumonia and decreased time to first mobilization with peripheral nerve block (single-shot blocks).[119]Guay J, Kopp S. Peripheral nerve blocks for hip fractures in adults. Cochrane Database Syst Rev. 2020 Nov 25;11(11):CD001159.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001159.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/33238043?tool=bestpractice.com
Opioid alternatives, both pharmacologic (e.g., nonsteroidal anti-inflammatory drugs [NSAIDs], acetaminophen) and nonpharmacologic (e.g., transcutaneous electrical stimulation, ice, cognitive therapies) should be considered alongside opioid-sparing protocols when possible given the risks of opioid analgesics (adverse events, misuse, opioid use disorder, and diversion for nonmedical use).[120]Hsu JR, Mir H, Wally MK, et al. Clinical practice guidelines for pain management in acute musculoskeletal injury. J Orthop Trauma. 2019 May;33(5):e158-82.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6485308
http://www.ncbi.nlm.nih.gov/pubmed/30681429?tool=bestpractice.com
[121]Ameican College of Surgeons. Best practices for acute pain management in trauma patients. Nov 2020 [internet publication].
https://www.facs.org/media/exob3dwk/acute_pain_guidelines.pdf
[122]Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016 Feb;17(2):131-57.
https://www.jpain.org/article/S1526-5900(15)00995-5/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/26827847?tool=bestpractice.com
Physical therapy and rehabilitation
Patients are generally prescribed physical therapy and rehabilitation; weight-bearing and range-of-motion activities are usually at the discretion of the treating surgeon. Based on limited evidence, the AAOS suggests consideration of immediate, full weight-bearing to tolerance.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Interdisciplinary care programs should be used in the care of patients with hip fractures to decrease complications and improve outcomes.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
This may include geriatric and orthopedic providers, alongside nursing, dietary, and rehabilitation providers such as occupational and physical therapists.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Coordinated multidisciplinary rehabilitation programs may result in an increased percentage of patients returning home and remaining there following a hip fracture.[114]Cameron ID. Coordinated multidisciplinary rehabilitation after hip fracture. Disabil Rehabil. 2005 Sep 30-Oct 15;27(18-19):1081-90.
http://www.ncbi.nlm.nih.gov/pubmed/16315427?tool=bestpractice.com
[123]Momsen AM, Rasmussen JO, Nielsen CV, et al. Multidisciplinary team care in rehabilitation: an overview of reviews. J Rehabil Med. 2012 Nov;44(11):901-12.
https://www.medicaljournals.se/jrm/content/html/10.2340/16501977-1040
http://www.ncbi.nlm.nih.gov/pubmed/23026978?tool=bestpractice.com
[124]Handoll HH, Cameron ID, Mak JC, et al. Multidisciplinary rehabilitation for older people with hip fractures. Cochrane Database Syst Rev. 2021 Nov 12;11(11):CD007125.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007125.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/34766330?tool=bestpractice.com
Specifically, patients monitored by a geriatrician postoperatively and given frequent physical therapy and occupational therapy in an acute care or rehabilitation setting may experience improved recovery of ambulatory and functional ability.[125]Chudyk AM, Jutai JW, Petrella RJ, et al. Systematic review of hip fracture rehabilitation practices in the elderly. Arch Phys Med Rehabil. 2009 Feb;90(2):246-62.
http://www.ncbi.nlm.nih.gov/pubmed/19236978?tool=bestpractice.com
[126]Prestmo A, Hagen G, Sletvold O, et al. Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial. Lancet. 2015 Apr 25;385(9978):1623-33.
http://www.ncbi.nlm.nih.gov/pubmed/25662415?tool=bestpractice.com
Use of clinical care pathways may be associated with a shorter length of hospital stay.[114]Cameron ID. Coordinated multidisciplinary rehabilitation after hip fracture. Disabil Rehabil. 2005 Sep 30-Oct 15;27(18-19):1081-90.
http://www.ncbi.nlm.nih.gov/pubmed/16315427?tool=bestpractice.com
Implementation of comprehensive geriatric assessment (CGA) programs may be of benefit in the perioperative period. CGAs are a coordinated, multidisciplinary assessment of the medical, psychosocial, and functional capabilities and limitations of older patients, and have been shown to improve outcomes (mortality, length of stay, re-admission, cost, discharge to an increased level of care) in people with hip fracture.[127]Eamer G, Taheri A, Chen SS, et al. Comprehensive geriatric assessment for older people admitted to a surgical service. Cochrane Database Syst Rev. 2018 Jan 31;(1):CD012485.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD012485.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/29385235?tool=bestpractice.com
There is limited evidence that home rehabilitation post-discharge improves long-term outcomes.[128]Crotty M, Unroe K, Cameron ID, et al. Rehabilitation interventions for improving physical and psychosocial functioning after hip fracture in older people. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007624.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007624.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/20091644?tool=bestpractice.com
There is some suggestion that extended rehabilitation may be beneficial.[129]Auais MA, Eilayyan O, Mayo NE. Extended exercise rehabilitation after hip fracture improves patients' physical function: a systematic review and meta-analysis. Phys Ther. 2012 Nov;92(11):1437-51.
http://www.ncbi.nlm.nih.gov/pubmed/22822235?tool=bestpractice.com
Dietary supplementation
There is low-quality evidence that oral multinutrient supplements (nonprotein energy, protein, vitamins, and minerals) started before or soon after surgery may prevent complications within the first 12 months after hip fracture, with no clear effect on mortality.[130]Avenell A, Smith TO, Curtain JP, et al. Nutritional supplementation for hip fracture aftercare in older people. Cochrane Database Syst Rev. 2016 Nov 30;(11):CD001880.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001880.pub6/full
http://www.ncbi.nlm.nih.gov/pubmed/27898998?tool=bestpractice.com
[  ]
For older adults recovering from hip fracture surgery, what are the effects of multinutrient supplements?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.2174/fullShow me the answer
]
For older adults recovering from hip fracture surgery, what are the effects of multinutrient supplements?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.2174/fullShow me the answer
Some studies have assessed the use of anabolic steroids, separately or in combination with nutritional supplements, after surgical treatment of patients with geriatric hip fracture; however, there is insufficient evidence to determine their effect.[131]Farooqi V, van den Berg ME, Cameron ID, et al. Anabolic steroids for rehabilitation after hip fracture in older people. Cochrane Database Syst Rev. 2014 Oct 6;(10):CD008887.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008887.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/25284341?tool=bestpractice.com
Wound coverage
Wound coverage within 7 days from injury date is recommended by the AAOS.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
After closed fracture fixation, negative-pressure wound therapy may mitigate the risk of revision surgery or surgical-site infections for higher-energy injuries with internal degloving (i.e., Morel-Lavallée lesions), or in patients with elevated body mass index; however, after open fracture fixation, negative-pressure wound therapy does not appear to offer an advantage when compared with sealed dressings as it does not decrease wound complications or amputations.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
Silver-coated dressings are not recommended as they do not improve outcomes or decrease pin-site infections.[57]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: evidence-based clinical practice guideline. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumacpg.pdf
[58]American Academy of Orthopaedic Surgeons. Prevention of surgical site infections after major extremity trauma: appropriate use criteria. March 2022 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/dod/ssitrauma/ssitraumaauc.pdf
Preoperative traction
Preoperative traction, including both skin and skeletal traction, should not be routinely used.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
Preoperative traction provides no benefit with regard to pain, ease of obtaining a reduction, or the quality of the reduction at the time of surgery.[17]American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. December 2021 [internet publication].
https://www.aaos.org/globalassets/quality-and-practice-resources/hip-fractures-in-the-elderly/hipfxcpg.pdf
[60]Mak JC, Cameron ID, March LM; National Health and Medical Research Council (Australia). Evidence-based guidelines for the management of hip fractures in older persons: an update. Med J Aust. 2010 Jan 4;192(1):37-41.
http://www.ncbi.nlm.nih.gov/pubmed/20047547?tool=bestpractice.com
[132]Handoll HH, Queally JM, Parker MJ. Pre-operative traction for hip fractures in adults. Cochrane Database Syst Rev. 2011 Dec 7;(12):CD000168.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000168.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/22161361?tool=bestpractice.com